

Evolving concepts in melanoma classification and their relevance to multidisciplinary melanoma patient care
- PMID: 21482206
- PMCID: PMC5528281
- DOI: 10.1016/j.molonc.2011.03.002
Evolving concepts in melanoma classification and their relevance to multidisciplinary melanoma patient care
Abstract
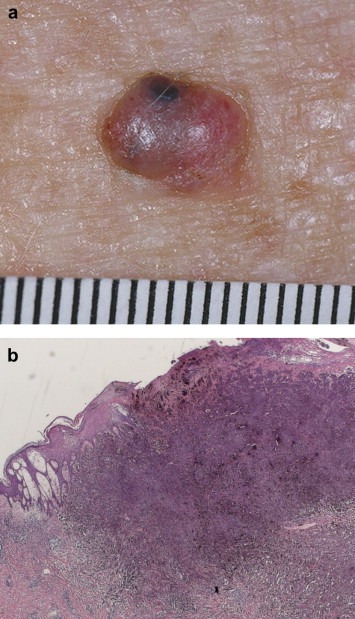
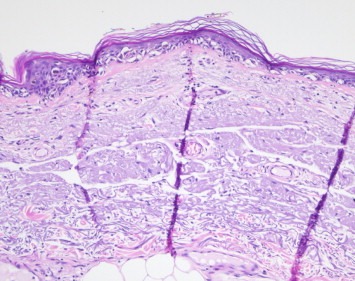
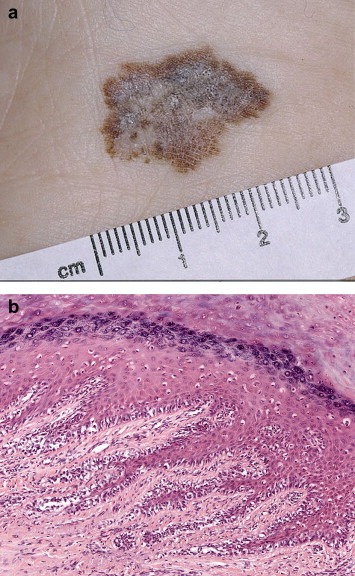
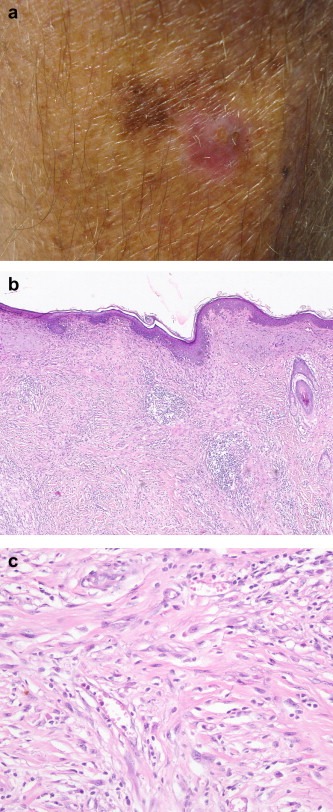
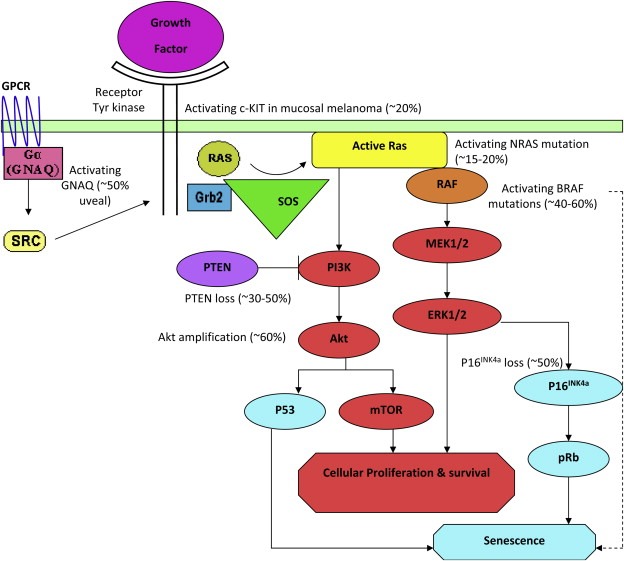
In the initial period after melanoma was recognised as a disease entity in the early 1800's, it was subclassified on the basis of its presumed origin (from a precursor naevus, from a melanocytic precursor lesion acquired during adult life or in previously blemish-fee skin). In 1967 the eminent American pathologist, Dr Wallace Clark, proposed a histogenetic classification for melanoma in which the disease was subdivided predominantly on the basis of histopathological features of the intra-epidermal component of the tumour adjacent to any dermal invasive component. The subtypes were superficial spreading melanoma (SSM), lentigo maligna melanoma (LMM) and nodular melanoma (NM). Whilst additional entities, including acral lentiginous melanoma, mucosal melanoma, desmoplastic melanoma and naevoid melanoma have since been recognised, SSM, LMM and NM remain in the latest (2006) version of the WHO melanoma classification. Clark's histogenetic classification has been criticised because the criteria upon which it is based include clinical features (such as the site of the melanoma) and non-tumourous histopathological features (such as the character of the associated epidermis and the degree of solar elastosis) and also because of overlap in defining features, lack of an independent association with patient outcome and minimal relevance as a determinant of clinical management. However, such criticisms fail to acknowledge its importance in highlighting the myriad of clinical and histological guises of melanoma, which if not recognized by clinicians and pathologists will inevitably lead to a delay in diagnosis and a concomitant adverse clinical outcome. Recently, mutually exclusive oncogenic mutations in melanomas involving NRAS (15-20%), BRAF (50%), CKIT (2%), and GNAQ/GNA11 (50% of uveal melanomas) have been identified. This might herald the beginning of a new molecular classification of melanoma in which the biologically distinct subsets share a common oncogenic mechanism, behave clinically in a similar fashion and require similar clinical management. These discoveries are already being successfully exploited as therapeutic targets in clinical trials of metastatic melanoma patients with promising activity. Whilst there remains much to be discovered in this rapidly evolving field, there is already great optimism that more rational and effective therapies for melanoma patients will soon be widely available.
Crown Copyright © 2011. Published by Elsevier B.V. All rights reserved.
Figures

References
-
- Allen, A.C. , Spitz, S. , 1953. Malignant melanoma; a clinicopathological analysis of the criteria for diagnosis and prognosis. Cancer. 6, 1–45. - PubMed
-
- Arrington, J.H. , Reed, R.J. , Ichinose, H. , Krementz, E.T. , 1977. Plantar lentiginous melanoma: a distinctive variant of human cutaneous malignant melanoma. Am. J. Surg. Pathol.. 1, 131–143. - PubMed
-
- Azzola, M.F. , Shaw, H.M. , Thompson, J.F. , Soong, S.J. , Scolyer, R.A. , Watson, G.F. , Colman, M.H. , Zhang, Y. , 2003. Tumor mitotic rate is a more powerful prognostic indicator than ulceration in patients with primary cutaneous melanoma: an analysis of 3661 patients from a single center. Cancer. 97, 1488–1498. - PubMed
-
- Balch, C.M. , Gershenwald, J.E. , Soong, S.J. , Thompson, J.F. , Atkins, M.B. , Byrd, D.R. , Buzaid, A.C. , Cochran, A.J. , Coit, D.G. , Ding, S. , Eggermont, A.M. , Flaherty, K.T. , Gimotty, P.A. , Kirkwood, J.M. , McMasters, K.M. , Mihm, M.C. , Morton, D.L. , Ross, M.I. , Sober, A.J. , Sondak, V.K. , 2009. Final version of 2009 AJCC melanoma staging and classification. J. Clin. Oncol.. 27, 6199–6206. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
