

Harnessing neuroplasticity for clinical applications
- PMID: 21482550
- PMCID: PMC3102236
- DOI: 10.1093/brain/awr039
Harnessing neuroplasticity for clinical applications
Abstract
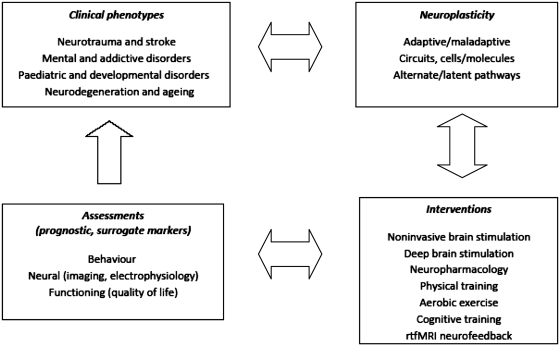
Neuroplasticity can be defined as the ability of the nervous system to respond to intrinsic or extrinsic stimuli by reorganizing its structure, function and connections. Major advances in the understanding of neuroplasticity have to date yielded few established interventions. To advance the translation of neuroplasticity research towards clinical applications, the National Institutes of Health Blueprint for Neuroscience Research sponsored a workshop in 2009. Basic and clinical researchers in disciplines from central nervous system injury/stroke, mental/addictive disorders, paediatric/developmental disorders and neurodegeneration/ageing identified cardinal examples of neuroplasticity, underlying mechanisms, therapeutic implications and common denominators. Promising therapies that may enhance training-induced cognitive and motor learning, such as brain stimulation and neuropharmacological interventions, were identified, along with questions of how best to use this body of information to reduce human disability. Improved understanding of adaptive mechanisms at every level, from molecules to synapses, to networks, to behaviour, can be gained from iterative collaborations between basic and clinical researchers. Lessons can be gleaned from studying fields related to plasticity, such as development, critical periods, learning and response to disease. Improved means of assessing neuroplasticity in humans, including biomarkers for predicting and monitoring treatment response, are needed. Neuroplasticity occurs with many variations, in many forms, and in many contexts. However, common themes in plasticity that emerge across diverse central nervous system conditions include experience dependence, time sensitivity and the importance of motivation and attention. Integration of information across disciplines should enhance opportunities for the translation of neuroplasticity and circuit retraining research into effective clinical therapies.
Figures
Comment in
-
Harnessing neuroplasticity for clinical applications.Brain. 2012 Apr;135(Pt 4):e215; author reply e216. doi: 10.1093/brain/aws017. Epub 2012 Feb 28. Brain. 2012. PMID: 22374936 Free PMC article. No abstract available.
References
-
- Awaya S. Stimulus deprivation amblyopia in humans. In: Reinecke R, editor. Strabismus. New York: Grune and Stratton; 1987.
-
- Aylward EH, Richards TL, Berninger VW, Nagy WE, Field KM, Grimme AC, et al. Instructional treatment associated with changes in brain activation in children with dyslexia. Neurology. 2003;61:212–9. - PubMed
-
- Bagati D, Nizamie SH, Prakash R. Effect of augmentatory repetitive transcranial magnetic stimulation on auditory hallucinations in schizophrenia: randomized controlled study. Aust N Z J Psychiatry. 2009;43:386–92. - PubMed
-
- Baillieux H, De Smet HJ, Dobbeleir A, Paquier PF, De Deyn PP, Marien P. Cognitive and affective disturbances following focal cerebellar damage in adults: a neuropsychological and SPECT study. Cortex. 2010;46:869–79. - PubMed
