

Postoperative radiotherapy for resected pathological stage IIIA-N2 non-small cell lung cancer: a retrospective study of 221 cases from a single institution
- PMID: 21482587
- PMCID: PMC3228200
- DOI: 10.1634/theoncologist.2010-0343
Postoperative radiotherapy for resected pathological stage IIIA-N2 non-small cell lung cancer: a retrospective study of 221 cases from a single institution
Abstract
Background: For patients with resected pathological stage IIIA-N2 non-small cell lung cancer (NSCLC), the role of postoperative radiotherapy (PORT) is not well defined. In this single-institutional study, we re-evaluated the effect of PORT on overall survival (OS) as well as tumor control in this subgroup of patients.
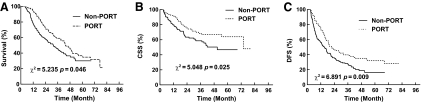
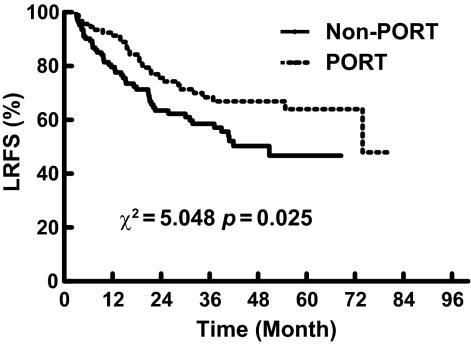
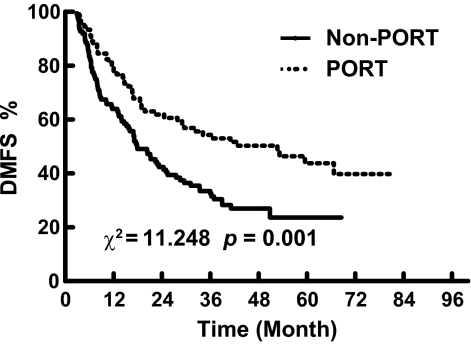
Methods: In 2003-2005, 221 consecutive patients with resected pathological stage IIIA-N2 NSCLC at our institution were retrospectively analyzed in an institutional review board-approved study. The effect of PORT on OS, cancer-specific survival (CSS), and disease-free survival (DFS) was evaluated using the Kaplan-Meier method and log-rank tests. The impact of PORT on locoregional control and distant metastasis was also analyzed. Results. Compared with the control, patients treated with PORT had a significantly longer OS time (χ2, 3.966; p = .046) and DFS interval (χ2, 6.891; p = .009), as well as a trend toward a longer CSS duration (χ2, 3.486; p = .062). Patients treated with PORT also had a significantly higher locoregional recurrence-free survival rate (χ2, 5.048; p = .025) as well as distant metastasis-free survival rate (χ2, 11.248; p = .001). Multivariate analyses showed that PORT was significantly associated with a longer OS duration (p = .000).
Conclusions: PORT can significantly improve the survival of patients with resected pathological stage IIIA-N2 NSCLC. A prospective randomized multicenter clinical trial is ongoing.
Conflict of interest statement
Section Editor
Section Editor
Reviewer “A” discloses research funding from Merck.
Reviewer “B” discloses no financial relationships.
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. On the basis of disclosed information, all conflicts of interest have been resolved.
Figures
References
-
- Vansteenkiste JF, De Leyn PP, Deneffe GJ, et al. Clinical prognostic factors in surgically treated stage IIIA-N2 non-small cell lung cancer: Analysis of the literature. Lung Cancer. 1998;19:3–13. - PubMed
-
- Suzuki K, Nagai K, Yoshida J, et al. The prognosis of surgically resected N2 non-small cell lung cancer: The importance of clinical N status. J Thorac Cardiovasc Surg. 1999;118:145–153. - PubMed
-
- Kim KJ, Ahn YC, Lim do H, et al. Analyses on prognostic factors following tri-modality therapy for stage IIIa non-small cell lung cancer. Lung Cancer. 2007;55:329–336. - PubMed
-
- Martini N, Flehinger BJ. The role of surgery in N2 lung cancer. Surg Clin North Am. 1987;67:1037–1049. - PubMed
-
- Casali C, Stefani A, Natali P, et al. Prognostic factors in surgically resected N2 non-small cell lung cancer: The importance of patterns of mediastinal lymph nodes metastases. Eur J Cardiothorac Surg. 2005;28:33–38. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
