

Detection of chronic kidney disease with creatinine, cystatin C, and urine albumin-to-creatinine ratio and association with progression to end-stage renal disease and mortality
- PMID: 21482744
- PMCID: PMC3697771
- DOI: 10.1001/jama.2011.468
Detection of chronic kidney disease with creatinine, cystatin C, and urine albumin-to-creatinine ratio and association with progression to end-stage renal disease and mortality
Abstract
Context: A triple-marker approach for chronic kidney disease (CKD) evaluation has not been well studied.
Objective: To evaluate whether combining creatinine, cystatin C, and urine albumin-to-creatinine ratio (ACR) would improve identification of risks associated with CKD compared with creatinine alone.
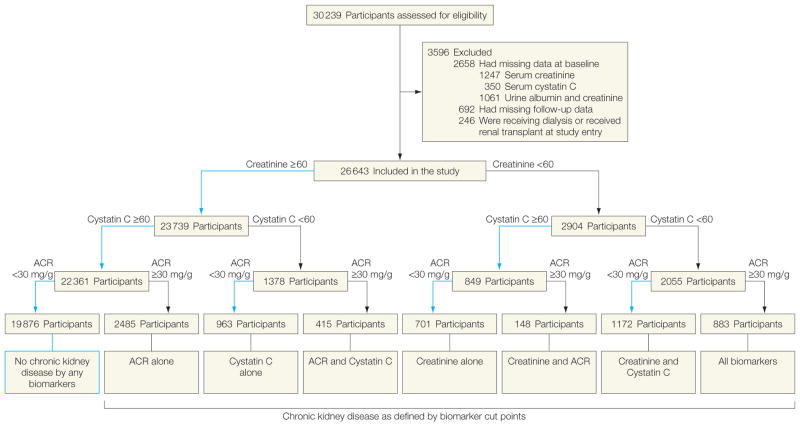
Design, setting, and participants: Prospective cohort study involving 26,643 US adults enrolled in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study from January 2003 to June 2010. Participants were categorized into 8 groups defined by estimated glomerular filtration rate (GFR) determined by creatinine and by cystatin C of either <60 or ≥60 mL/min/1.73 m(2) and ACR of either <30 or ≥30 mg/g.
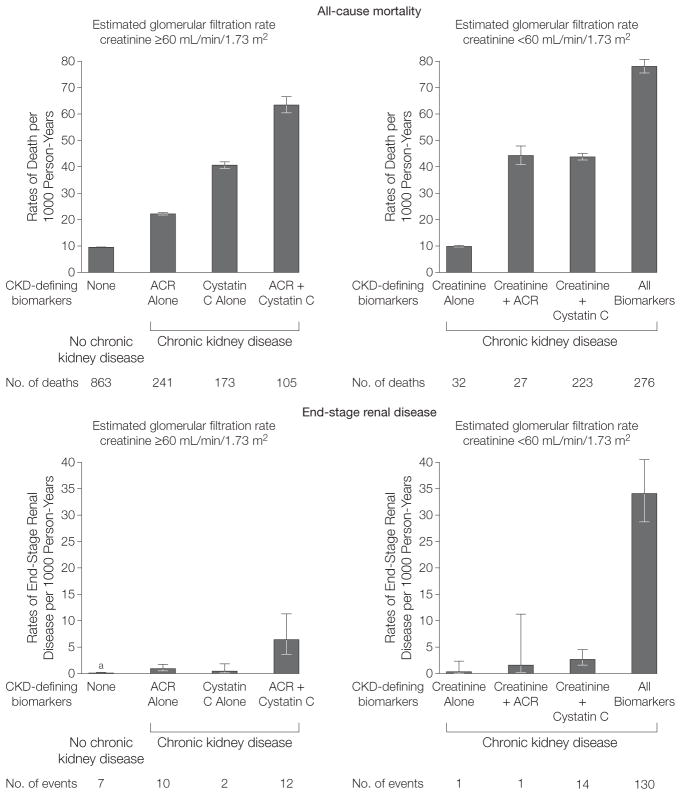
Main outcome measures: All-cause mortality and incident end-stage renal disease with median follow-up of 4.6 years.
Results: Participants had a mean age of 65 years, 40% were black, and 54% were women. Of 26,643 participants, 1940 died and 177 developed end-stage renal disease. Among participants without CKD defined by creatinine, 24% did not have CKD by either ACR or cystatin C. Compared with those with CKD defined by creatinine alone, the hazard ratio for death in multivariable-adjusted models was 3.3 (95% confidence interval [CI], 2.0-5.6) for participants with CKD defined by creatinine and ACR; 3.2 (95% CI, 2.2-4.7) for those with CKD defined by creatinine and cystatin C, and 5.6 (95% CI, 3.9-8.2) for those with CKD defined by all biomarkers. Among participants without CKD defined by creatinine, 3863 (16%) had CKD detected by ACR or cystatin C. Compared with participants who did not have CKD by any measure, the HRs for mortality were 1.7 (95% CI, 1.4-1.9) for participants with CKD defined by ACR alone, 2.2 (95% CI, 1.9-2.7) for participants with CKD defined by cystatin C alone, and 3.0 (95% CI, 2.4-3.7) for participants with CKD defined by both measures. Risk of incident end-stage renal disease was higher among those with CKD defined by all markers (34.1 per 1000 person-years; 95% CI, 28.7-40.5 vs 0.33 per 1000 person-years; 95% CI, 0.05-2.3) for those with CKD defined by creatinine alone. The second highest end-stage renal disease rate was among persons missed by the creatinine measure but detected by both ACR and cystatin C (rate per 1000 person-years, 6.4; 95% CI, 3.6-11.3). Net reclassification improvement for death was 13.3% (P < .001) and for end-stage renal disease was 6.4% (P < .001) after adding estimated GFR cystatin C in fully adjusted models with estimated GFR creatinine and ACR.
Conclusion: Adding cystatin C to the combination of creatinine and ACR measures improved the predictive accuracy for all-cause mortality and end-stage renal disease.
Conflict of interest statement
Figures
Comment in
-
Supplementing creatinine-based estimates of risk in chronic kidney disease: is it time?JAMA. 2011 Apr 20;305(15):1593-5. doi: 10.1001/jama.2011.502. Epub 2011 Apr 11. JAMA. 2011. PMID: 21482745 No abstract available.
-
Chronic kidney disease: Use of urine albumin and cystatin C levels improves risk stratification in chronic kidney disease.Nat Rev Nephrol. 2011 Jun;7(6):301. doi: 10.1038/nrneph.2011.47. Nat Rev Nephrol. 2011. PMID: 21625199 No abstract available.
-
Biomarkers for detecting and risk-stratifying chronic kidney disease.JAMA. 2011 Aug 10;306(6):611; author reply 611-2. doi: 10.1001/jama.2011.1111. JAMA. 2011. PMID: 21828322 No abstract available.
-
Biomarkers for detecting and risk-stratifying chronic kidney disease.JAMA. 2011 Aug 10;306(6):611; author reply 611-2. doi: 10.1001/jama.2011.1110. JAMA. 2011. PMID: 21828323 No abstract available.
References
-
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 suppl 1):S1–S266. - PubMed
-
- Molitch ME, DeFronzo RA, Franz MJ, et al. American Diabetes Association. Nephropathy in diabetes. Diabetes Care. 2004;27(suppl 1):S79–S83. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305. - PubMed
-
- Menon V, Wang X, Sarnak MJ, et al. Long-term outcomes in nondiabetic chronic kidney disease. Kidney Int. 2008;73(11):1310–1315. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01AG034853/AG/NIA NIH HHS/United States
- R01 HL085757/HL/NHLBI NIH HHS/United States
- 1K23SK082793-01/PHS HHS/United States
- R01 DK078124/DK/NIDDK NIH HHS/United States
- R01DK066488/DK/NIDDK NIH HHS/United States
- R03 DK095877/DK/NIDDK NIH HHS/United States
- R01HL085757/HL/NHLBI NIH HHS/United States
- K23 DK082793/DK/NIDDK NIH HHS/United States
- R01 DK066488/DK/NIDDK NIH HHS/United States
- U01 NS041588/NS/NINDS NIH HHS/United States
- R01 HL080477/HL/NHLBI NIH HHS/United States
- R01DK078124/DK/NIDDK NIH HHS/United States
- R21 HL091217/HL/NHLBI NIH HHS/United States
- R21HL091217/HL/NHLBI NIH HHS/United States
- R01 AG034853/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
