

Anti-ErbB-2 mAb therapy requires type I and II interferons and synergizes with anti-PD-1 or anti-CD137 mAb therapy
- PMID: 21482773
- PMCID: PMC3084100
- DOI: 10.1073/pnas.1016569108
Anti-ErbB-2 mAb therapy requires type I and II interferons and synergizes with anti-PD-1 or anti-CD137 mAb therapy
Abstract
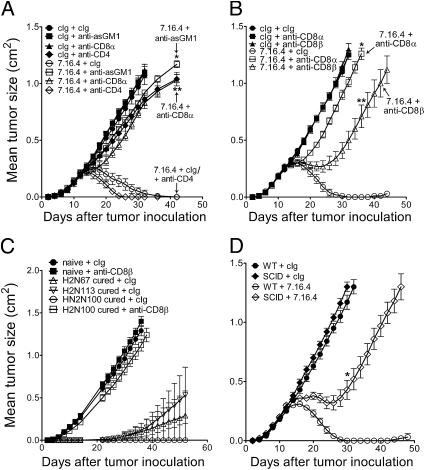
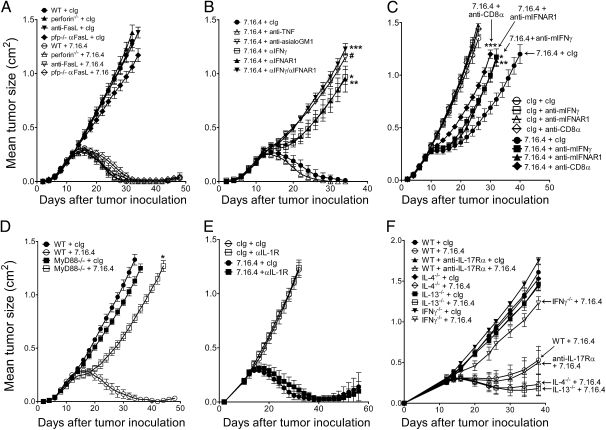
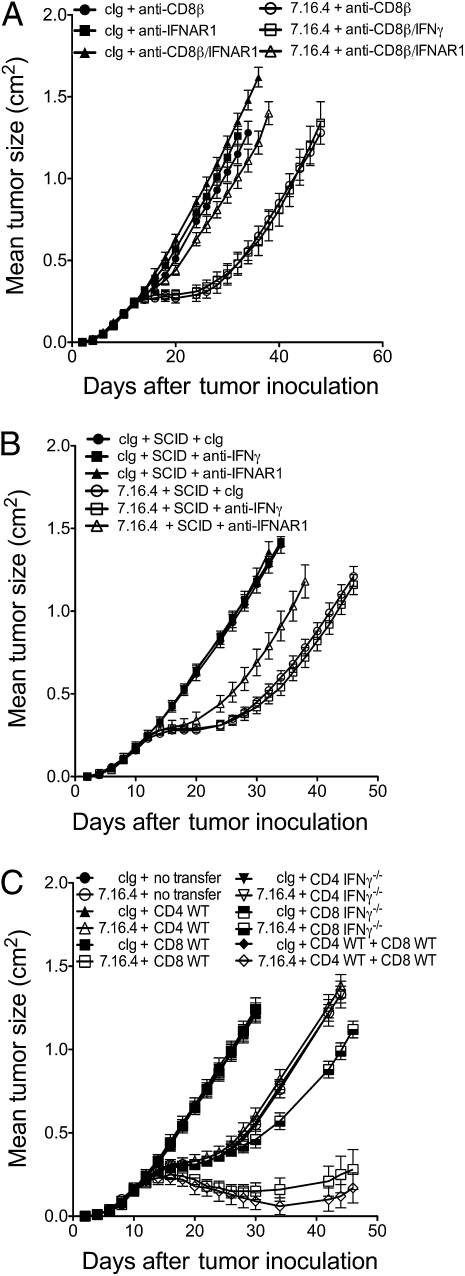
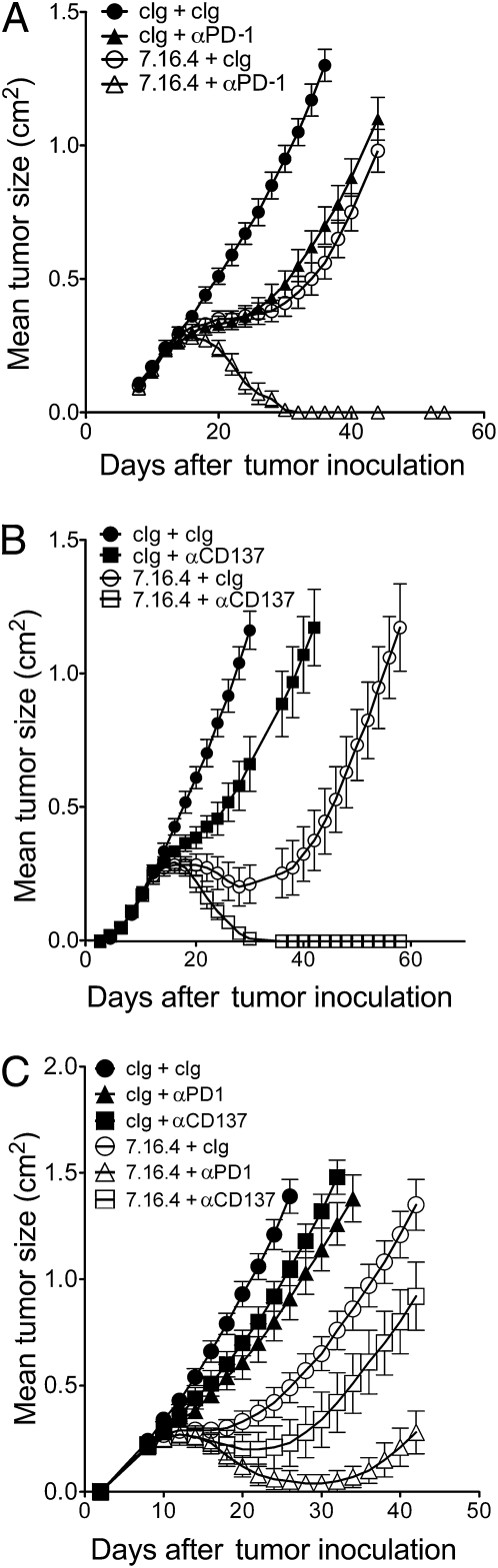
Trastuzumab, a monoclonal antibody targeting human epidermal growth factor receptor-2 (HER2/ErbB-2), has become the mainstay of treatment for HER2-positive breast cancer. Nevertheless, its exact mechanism of action has not been fully elucidated. Although several studies suggest that Fc receptor-expressing immune cells are involved in trastuzumab therapy, the relative contribution of lymphocyte-mediated cellular cytotoxicity and antitumor cytokines remains unknown. We report here that anti-ErbB-2 mAb therapy is dependent on the release of type I and type II IFNs but is independent of perforin or FasL. Our study thus challenges the notion that classical antibody-dependent, lymphocyte-mediated cellular cytotoxicity is important for trastuzumab. We demonstrate that anti-ErbB-2 mAb therapy of experimental tumors derived from MMTV-ErbB-2 transgenic mice triggers MyD88-dependent signaling and primes IFN-γ-producing CD8+ T cells. Adoptive cell transfer of purified T cell subsets confirmed the essential role of IFN-γ-producing CD8+ T cells. Notably, anti-ErbB-2 mAb therapy was independent of IL-1R or IL-17Ra signaling. Finally, we investigated whether immunostimulatory approaches with antibodies against programmed death-1 (PD-1) or 41BB (CD137) could be used to capitalize on the immune-mediated effects of trastuzumab. We demonstrate that anti-PD-1 or anti-CD137 mAb can significantly improve the therapeutic activity of anti-ErbB-2 mAb in immunocompetent mice.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Hudis CA. Trastuzumab—mechanism of action and use in clinical practice. N Engl J Med. 2007;357:39–51. - PubMed
-
- Spector NL, Blackwell KL. Understanding the mechanisms behind trastuzumab therapy for human epidermal growth factor receptor 2-positive breast cancer. J Clin Oncol. 2009;27:5838–5847. - PubMed
-
- Untch M, et al. Neoadjuvant treatment with trastuzumab in HER2-positive breast cancer: Results from the GeparQuattro study. J Clin Oncol. 2010;28:2024–2031. - PubMed
-
- Clynes RA, Towers TL, Presta LG, Ravetch JV. Inhibitory Fc receptors modulate in vivo cytoxicity against tumor targets. Nat Med. 2000;6:443–446. - PubMed
-
- Musolino A, et al. Immunoglobulin G fragment C receptor polymorphisms and clinical efficacy of trastuzumab-based therapy in patients with HER-2/neu-positive metastatic breast cancer. J Clin Oncol. 2008;26:1789–1796. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
