

Epidemiology and natural history of intestinal metaplasia of the gastroesophageal junction and Barrett's esophagus: a population-based study
- PMID: 21483461
- PMCID: PMC3150349
- DOI: 10.1038/ajg.2011.130
Epidemiology and natural history of intestinal metaplasia of the gastroesophageal junction and Barrett's esophagus: a population-based study
Abstract
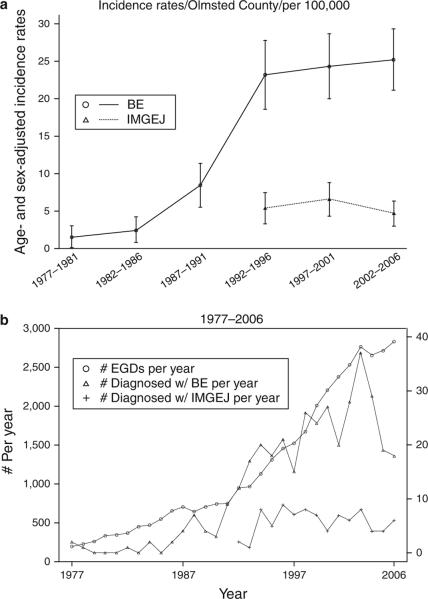
Objectives: Population-based data on the epidemiology and outcomes of subjects with intestinal metaplasia of the gastroesophageal junction (IMGEJ) and Barrett's esophagus (BE) are limited. The objectives of this study were to (i) estimate the incidence of IMGEJ and BE diagnosed from clinically indicated endoscopy in Olmsted County, MN, over three decades (1976-2006) and prevalence as of 1 January 2007, (ii) compare baseline characteristics of subjects with IMGEJ and BE, and (iii) study the natural history and survival of both cohorts.
Methods: This was a population-based cohort study. The study setting was Olmsted County, MN. Patients with BE (columnar segment >1 cm with intestinal metaplasia) and IMGEJ (intestinal metaplasia in biopsies from the gastroesophageal junction) from 1976 to 2006 in Olmsted County, MN, were identified using Rochester Epidemiology Project resources. Demographic and clinical data were abstracted from medical records and pathology confirmed by gastrointestinal pathologists. The association of baseline characteristics with overall and progression-free survival was assessed using proportional hazards regression models. Outcome measures were baseline characteristics and overall survival of subjects with IMGEJ compared to those with BE.
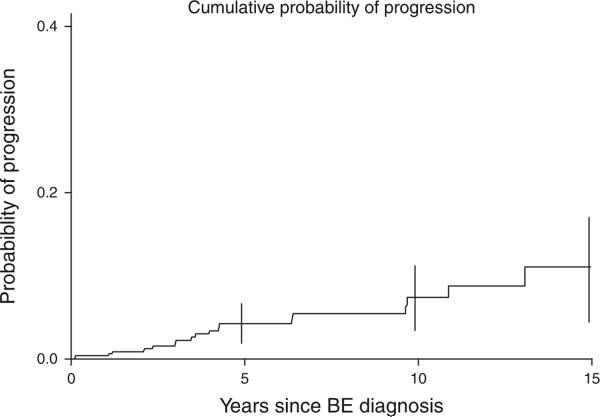
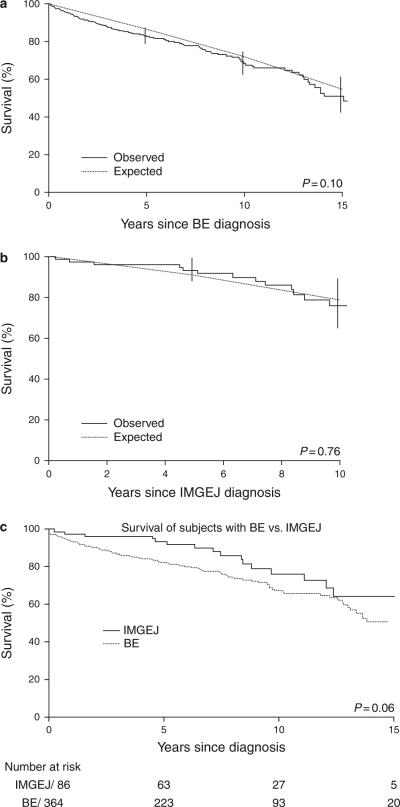
Results: In all, 487 patients (401 with BE and 86 with IMGEJ) were identified and followed for a median interval of 7 (BE subjects) to 8 (IMGEJ subjects) years. Subjects with BE were older, heavier, reported reflux symptoms more often, and had higher prevalence of advanced neoplasia than those with IMGEJ. No patient with IMGEJ progressed to esophageal adenocarcinoma (EAC) in contrast to BE subjects who had a cumulative risk of progression of 7% at 10 years and increased risk of death from EAC (standardized mortality ratio 9.62). The overall survival of subjects with BE and IMGEJ did not differ from that expected in similar age- and sex-distributed white Minnesota populations.
Conclusions: Subjects with IMGEJ appear to have distinct clinical characteristics and substantially lower cancer progression risk compared to those with BE.
Figures
References
-
- Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97:142–6. - PubMed
-
- Wang KK, Sampliner RE. Updated guidelines 2008 for the diagnosis, surveillance and therapy of Barrett's esophagus. Am J Gastroenterol. 2008;103:788–97. - PubMed
-
- Sharma P, Dent J, Armstrong D, et al. The development and validation of an endoscopic grading system for Barrett's esophagus: the Prague C & M criteria. Gastroenterology. 2006;131:1392–9. - PubMed
-
- Sharma P, McQuaid K, Dent J, et al. A critical review of the diagnosis and management of Barrett's esophagus: the AGA Chicago Workshop. Gastroenterology. 2004;127:310–30. - PubMed
-
- Chandrasoma P, Wickramasinghe K, Ma Y, et al. Adenocarcinomas of the distal esophagus and “gastric cardia” are predominantly esophageal carcinomas. Am J Surg Pathol. 2007;31:569–75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
