

Correlation between squamous suture and sylvian fissure: OSIRIX DICOM viewer study
- PMID: 21483821
- PMCID: PMC3069062
- DOI: 10.1371/journal.pone.0018199
Correlation between squamous suture and sylvian fissure: OSIRIX DICOM viewer study
Abstract
Background: Sylvian fissure (SF) is an important corridor in neurosurgery, and the end of sylvian fissure (eSF) represents the optimal target area to expose suitable recipient artery in STA-MCA bypass. Unfortunately little have been addressed concerning its relationship with external cranial surface.
Objective: Correlation between Squamous Suture (SS) and SF was investigated.
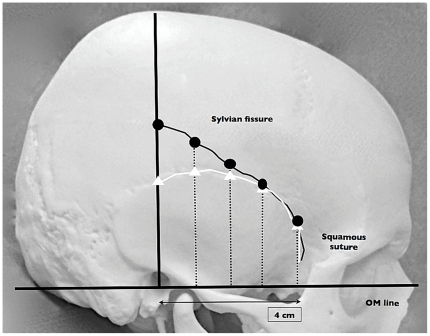
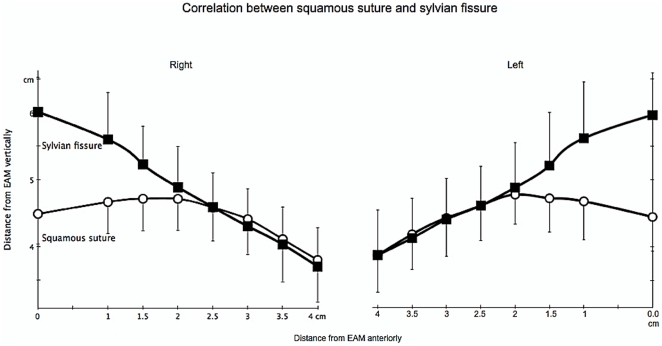
Methods: 50-adult 3D-CTA images were studied using OSIRIX DICOM viewer. The measurement points were determined from external auditory meatus 0, 1, 1.5, 2, 2.5, 3, 3.5 and 4-cm anteriorly, perpendicular from orbitomeatal (OM) line. The distance of SF was compared with the one of SS.
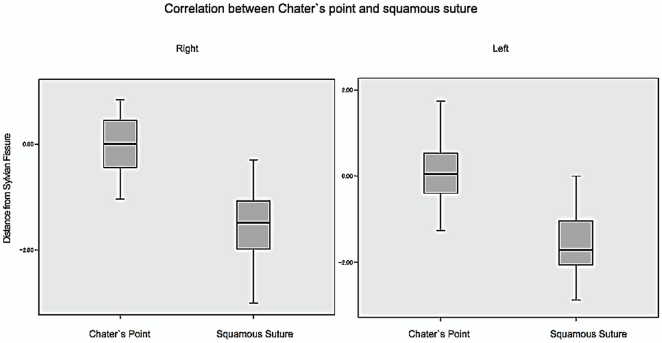
Results: SSs were all located below SF at 0 cm. At a distance of 0 to 1.5 cm, SSs were located above SF, then started to merge and went side by side from 2 cm anteriorly. Anterior sylvian point, the most anterior part of SF, was found at 4 cm from OM line. Inferior Rolandic point, which corresponds to the central sulcus inferior extent, was found to be at 2 cm from OM line. The eSF was identified at 0 cm anteriorly from OM, and perpendicularly 1.5 cm above SS. 50% patients had Chater's point (CP) above eSF. Average value for CP was 0.01 below eSF, giving a significantly closer value compared to the one of SS (p<0.01). However, SS showed consistent value of 1.5 below SF. Furthermore, SS is a bony landmark, which has no shifting effect during surgery, therefore drawing a 1.5-cm line upward from SS could lead to exact location of eSF.
Conclusion: The course of SF and its correlation to SS have been identified, and this is also the first study to investigate the relationship of SS and eSF using OSIRIX DICOM viewer. SS is also comparable to CP, therefore it is usable for a simple landmark of eSF.
Conflict of interest statement
Figures


Similar articles
-
Use of Three-Dimensional Curved-Multiplanar Reconstruction Images for Sylvian Dissection in Microsurgery of Middle Cerebral Artery Aneurysms.Yonsei Med J. 2017 Jan;58(1):241-247. doi: 10.3349/ymj.2017.58.1.241. Yonsei Med J. 2017. PMID: 27873519 Free PMC article.
-
Venous-Preserving Sylvian Dissection.World Neurosurg. 2015 Dec;84(6):2043-52. doi: 10.1016/j.wneu.2015.07.050. Epub 2015 Jul 29. World Neurosurg. 2015. PMID: 26232211
-
Dr. Norman Chater and Chater's Point.World Neurosurg. 2017 Oct;106:281-284. doi: 10.1016/j.wneu.2017.06.130. Epub 2017 Jun 28. World Neurosurg. 2017. PMID: 28666915
-
The microanatomy of the Sylvian fissure.Childs Nerv Syst. 2023 Jan;39(1):67-72. doi: 10.1007/s00381-022-05682-6. Epub 2022 Sep 26. Childs Nerv Syst. 2023. PMID: 36161522 Review.
-
OsiriX software as a preoperative planning tool in cranial neurosurgery: A step-by-step guide for neurosurgical residents.Surg Neurol Int. 2017 Oct 10;8:241. doi: 10.4103/sni.sni_419_16. eCollection 2017. Surg Neurol Int. 2017. PMID: 29119039 Free PMC article. Review.
Cited by
-
Superficial Temporal Artery-Sparing Mini-Pterional Approach for Cerebral Aneurysm Surgery.J Korean Neurosurg Soc. 2017 Jan 1;60(1):8-14. doi: 10.3340/jkns.2016.0707.004. Epub 2016 Dec 29. J Korean Neurosurg Soc. 2017. PMID: 28061486 Free PMC article.
-
Evaluation of 3-dimensional superimposition techniques on various skeletal structures of the head using surface models.PLoS One. 2015 Feb 23;10(2):e0118810. doi: 10.1371/journal.pone.0118810. eCollection 2015. PLoS One. 2015. PMID: 25706151 Free PMC article.
-
Skin landmarks to main cerebral structures: how to identify the main cerebral sulci? A radiological study about lateral, central, and parietooccipital sulci.Surg Radiol Anat. 2022 Jun;44(6):941-946. doi: 10.1007/s00276-022-02952-5. Epub 2022 May 8. Surg Radiol Anat. 2022. PMID: 35526190
-
The Use of Osirix for Surgical Planning Using Cranial Measures and Region of Interest Tools: Technical Note.Asian J Neurosurg. 2019 Jul-Sep;14(3):762-766. doi: 10.4103/ajns.AJNS_63_19. Asian J Neurosurg. 2019. PMID: 31497099 Free PMC article.
-
Morphology of the lateral fossa of the brain (sylvian valley): anatomo-radiological aspects and surgical application.Surg Radiol Anat. 2019 Jun;41(6):639-655. doi: 10.1007/s00276-019-02228-5. Epub 2019 Apr 6. Surg Radiol Anat. 2019. PMID: 30955058
References
-
- Yasargil MG. Thieme, Stuttgart; 1969. Microsurgery applied to neurosurgery. pp. 119–143.
-
- Aydin IH, Kadioğlu HH, Tüzün Y, Kayaoğlu CR, Takçi E. The variations of Sylvian veins and cisterns in anterior circulation aneurysms. An operative study. Acta Neurochir (Wien): 138(12); 1996;1380–1385 - PubMed
-
- Ebeling U, Steinmetz H, Huang YX, Kahn T. Topography and identification of the inferior precentral sulcus in MR imaging. AJR Am J Roentgenol: Nov;153(5); 1989;1051–1056 - PubMed
-
- Harkey HL, al-Mefty O, Haines DE, Smith RR. The surgical anatomy of the cerebral sulci. Neurosurgery: May;24(5); 1989;651–654 - PubMed
-
- Kazumata K, Kamiyama H, Ishikawa T, Takizawa K, Maeda T, et al. Operative anatomy and classification of the sylvian veins for the distal transsylvian approach. Neurol Med Chir (Tokyo): Sep;43(9); 2003;427–433 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
