

Previous lung diseases and lung cancer risk: a systematic review and meta-analysis
- PMID: 21483846
- PMCID: PMC3069026
- DOI: 10.1371/journal.pone.0017479
Previous lung diseases and lung cancer risk: a systematic review and meta-analysis
Abstract
Background: In order to review the epidemiologic evidence concerning previous lung diseases as risk factors for lung cancer, a meta-analysis and systematic review was conducted.
Methods: Relevant studies were identified through MEDLINE searches. Using random effects models, summary effects of specific previous conditions were evaluated separately and combined. Stratified analyses were conducted based on smoking status, gender, control sources and continent.
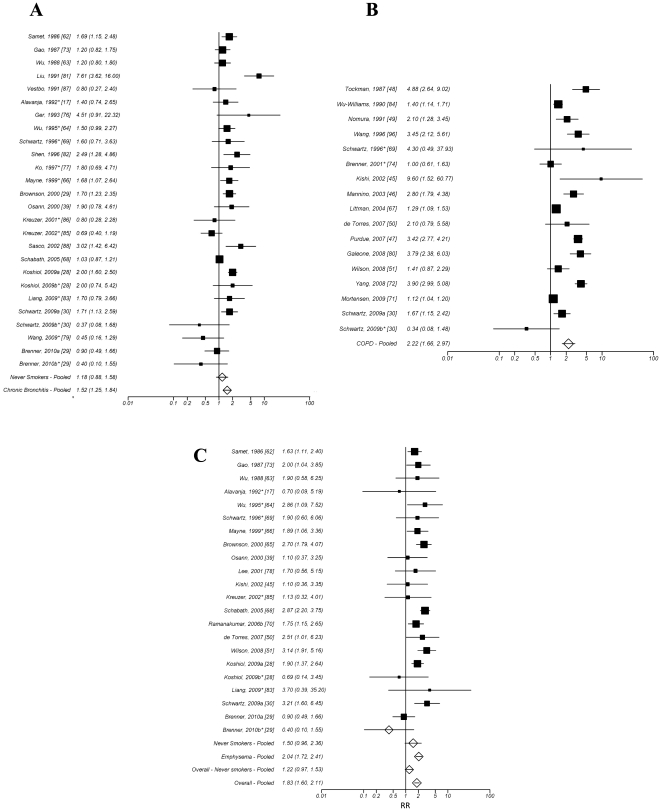
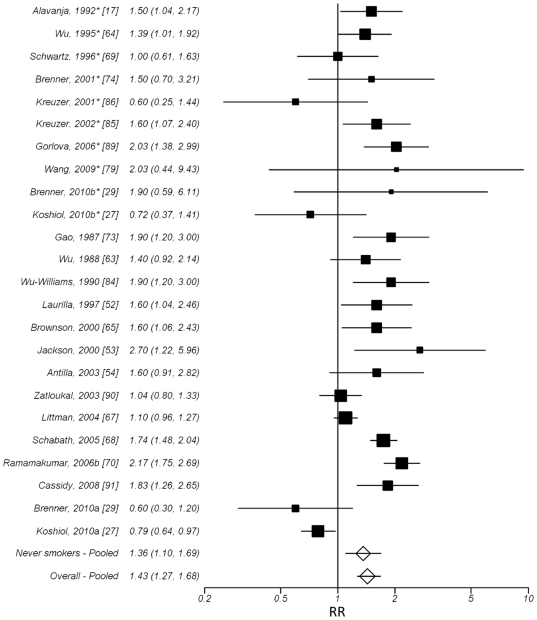
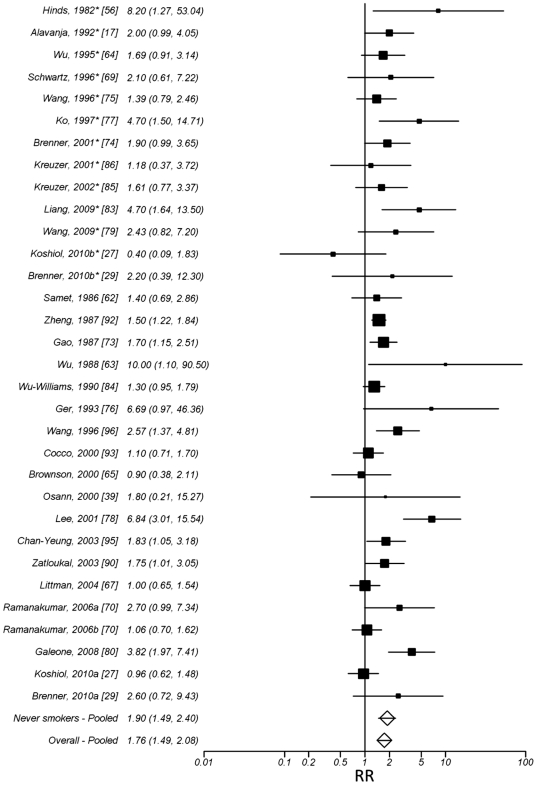
Results: A previous history of COPD, chronic bronchitis or emphysema conferred relative risks (RR) of 2.22 (95% confidence interval (CI): 1.66, 2.97) (from 16 studies), 1.52 (95% CI: 1.25, 1.84) (from 23 studies) and 2.04 (95% CI: 1.72, 2.41) (from 20 studies), respectively, and for all these diseases combined 1.80 (95% CI: 1.60, 2.11) (from 39 studies). The RR of lung cancer for subjects with a previous history of pneumonia was 1.43 (95% CI: 1.22-1.68) (from 22 studies) and for subjects with a previous history of tuberculosis was 1.76 (95% CI=1.49, 2.08), (from 30 studies). Effects were attenuated when restricting analysis to never smokers only for COPD/emphysema/chronic bronchitis (RR=1.22, 0.97-1.53), however remained significant for pneumonia 1.36 (95% CI: 1.10, 1.69) (from 8 studies) and tuberculosis 1.90 (95% CI: 1.45, 2.50) (from 11 studies).
Conclusions: Previous lung diseases are associated with an increased risk of lung cancer with the evidence among never smokers supporting a direct relationship between previous lung diseases and lung cancer.
Conflict of interest statement
Figures
References
-
- Stewart BW, Kleihues P, editors. Lyons, France: IARC Press; 2003. World Cancer Report.342
-
- Peek RM, Jr, Mohla S, DuBois RN. Inflammation in the genesis and perpetuation of cancer: summary and recommendations from a national cancer institute-sponsored meeting. Cancer Res. 2005;65:8583–8586. - PubMed
-
- Ballaz S, Mulshine JL. The potential contributions of chronic inflammation to lung carcinogenesis. Clin Lung Cancer. 2003;5:46–62. - PubMed
-
- Rakoff-Nahoum S, Medzhitov R. Toll-like receptors and cancer. Nat Rev Cancer. 2009;9:57–63. - PubMed
-
- Weitzman SA, Gordon LI. Inflammation and cancer: role of phagocyte-generated oxidants in carcinogenesis. Blood. 1990;76:655–663. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
