

Intermediate uveitis in Indian population
- PMID: 21484178
- PMCID: PMC3102854
- DOI: 10.1007/s12348-011-0020-3
Intermediate uveitis in Indian population
Abstract
Purpose: Intermediate uveitis (IU) is generally believed to be autoimmune in nature requiring systemic corticosteroid and immunomodulatory therapy. This belief stems from the published reports from the developed countries; and the scenario maybe different in the developing countries that maybe endemic for certain infections. There are no large series available on the etiologic causes of intermediate uveitis from the developing countries. The present series aims to describe the etiology, treatment, and course of IU in North Indian population.
Methods: In a retrospective analysis, records of 205 patients seen with a referral diagnosis of IU were retrieved and analyzed. After determining the etiology, 122 patients who had a definitive diagnosis of IU and a minimum follow-up of 1 year were analyzed further. All patients underwent investigations to rule out any possible etiology and received stepwise therapy comprising of depot or systemic corticosteroids, immunosuppressive/immunomodulatory therapy and pars plana vitrectomy. Specific therapy was administered wherever etiology could be determined. The primary outcome measure was recurrence of inflammation after a minimum of 6 months of initiating treatment.
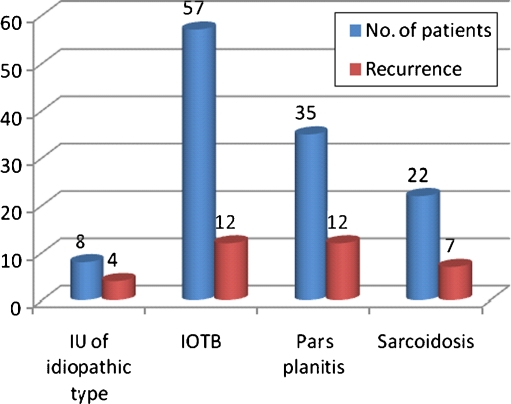
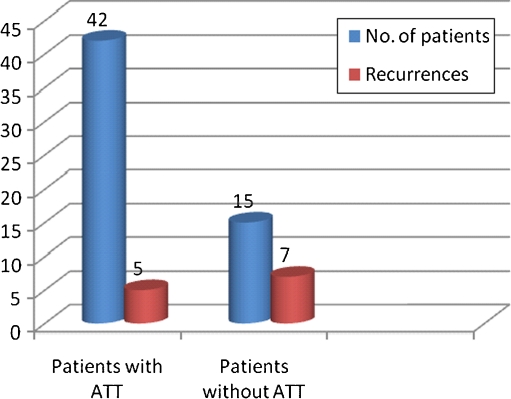
Results: There were 55 men and 67 women, and the disease was bilateral in 82 patients. Tuberculosis was the most common underlying etiology seen in 57 (46.7%), followed by sarcoidosis in 22 (18%), pars planitis in 35 (28.7%), and IU of idiopathic type in 8 (6.5%). Seventy three (59.8%) of 122 patients received systemic steroids, 55 (45.1%) were treated with periocular steroid, and 19 (15.6%) received immunomodulatory therapy. Specific antimicrobial therapy in the form of antitubercular treatment (ATT) was given in 42 patients. The recurrences were seen in 35 patients (28.7%) over a median follow-up of 18 months. Recurrences were seen more commonly in eyes with snow banking (P = 0.011); cystoid macular edema (P = 0.015), and in eyes that received local therapy (P = 0.001). Out of 57 patients who were diagnosed as intraocular tuberculosis, 42 patients (73.6%) received specific antitubercular treatment. Only 5 of 42 patients (11.9%) who received ATT had recurrence of inflammation compared to 7 out of 15 patients (46.7%) who did not receive ATT (P = 0.005).
Conclusions: Tuberculosis is an important etiologic cause of IU in developing countries like India where the disease is endemic. It is important to investigate these patients as specific therapy with ATT helped in reducing the recurrences significantly.
Figures
Similar articles
-
Unilateral snow banking in tuberculosis-related intermediate uveitis.J Ophthalmic Inflamm Infect. 2014 Feb 10;4(1):4. doi: 10.1186/1869-5760-4-4. J Ophthalmic Inflamm Infect. 2014. PMID: 24507077 Free PMC article.
-
Intermediate uveitis: pattern of etiology, complications, treatment and outcome in a tertiary academic center.Orphanet J Rare Dis. 2017 Apr 27;12(1):81. doi: 10.1186/s13023-017-0638-9. Orphanet J Rare Dis. 2017. PMID: 28449695 Free PMC article.
-
Intermediate Uveitis: A Review.Ocul Immunol Inflamm. 2023 Jul;31(5):1041-1060. doi: 10.1080/09273948.2022.2070503. Epub 2022 Jun 27. Ocul Immunol Inflamm. 2023. PMID: 35759636 Review.
-
Pars plana vitrectomy in patients with intermediate uveitis.Ocul Immunol Inflamm. 2001 Sep;9(3):141-51. doi: 10.1076/ocii.9.3.141.3965. Ocul Immunol Inflamm. 2001. PMID: 11815883
-
Pars Planitis: Epidemiology, Clinical Characteristics, Management and Visual Prognosis.J Ophthalmic Vis Res. 2015 Oct-Dec;10(4):469-80. doi: 10.4103/2008-322X.176897. J Ophthalmic Vis Res. 2015. PMID: 27051493 Free PMC article. Review.
Cited by
-
Prevalence, clinical profile, investigations, and visual outcome of sarcoid intermediate uveitis in a tertiary eye care center in South India.Indian J Ophthalmol. 2022 Jul;70(7):2454-2457. doi: 10.4103/ijo.IJO_3099_21. Indian J Ophthalmol. 2022. PMID: 35791132 Free PMC article.
-
Ocular tuberculosis: current perspectives.Clin Ophthalmol. 2015 Nov 26;9:2223-7. doi: 10.2147/OPTH.S65254. eCollection 2015. Clin Ophthalmol. 2015. PMID: 26648690 Free PMC article. Review.
-
Unilateral snow banking in tuberculosis-related intermediate uveitis.J Ophthalmic Inflamm Infect. 2014 Feb 10;4(1):4. doi: 10.1186/1869-5760-4-4. J Ophthalmic Inflamm Infect. 2014. PMID: 24507077 Free PMC article.
-
Clinical characteristics of intermediate uveitis in adults according to criteria of the SUN working group.Int Ophthalmol. 2023 Oct;43(10):3681-3693. doi: 10.1007/s10792-023-02778-z. Epub 2023 Jul 3. Int Ophthalmol. 2023. PMID: 37395903
-
Rare case of ocular tuberculosis in a diabetic patient: diagnostic and therapeutic dilemmas.Rom J Ophthalmol. 2017 Apr-Jun;61(2):137-143. doi: 10.22336/rjo.2017.26. Rom J Ophthalmol. 2017. PMID: 29450388 Free PMC article.
References
-
- Bloch-Michel E, Nussenblatt B. International uveitis study group recommendations for the evaluation of intraocular inflammatory disease. Am J Ophthalmol. 1987;103:234–235. - PubMed
-
- Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140:509–516. doi: 10.1016/j.ajo.2005.03.057. - DOI - PMC - PubMed
-
- Zierhut M, Foster CS. Multiple sclerosis, sarcoidosis, and other diseases in patients with pars planitis. Dev Ophthalmol. 1992;23:41–47. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
