

Disparities in post-acute rehabilitation care for joint replacement
- PMID: 21485020
- PMCID: PMC3128236
- DOI: 10.1002/acr.20477
Disparities in post-acute rehabilitation care for joint replacement
Abstract
Objective: To determine the extent to which demographic and geographic disparities exist in the use of post-acute rehabilitation care (PARC) for joint replacement.
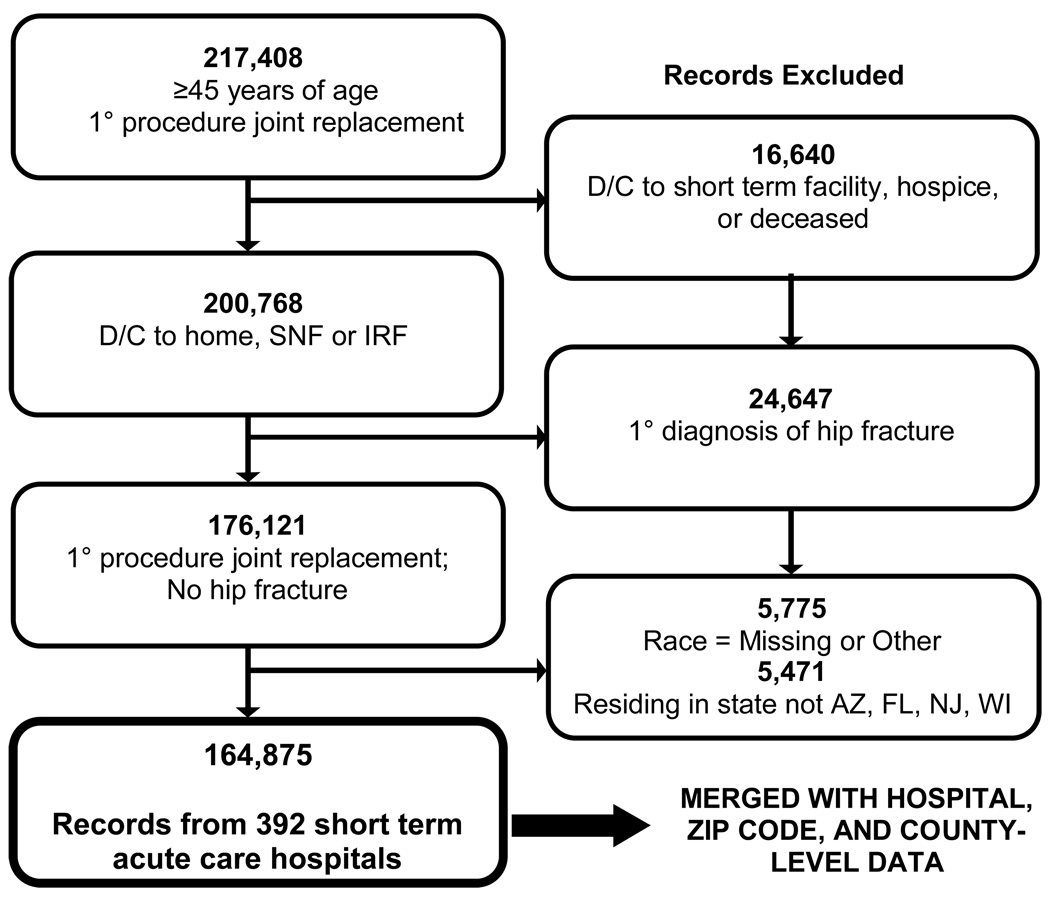
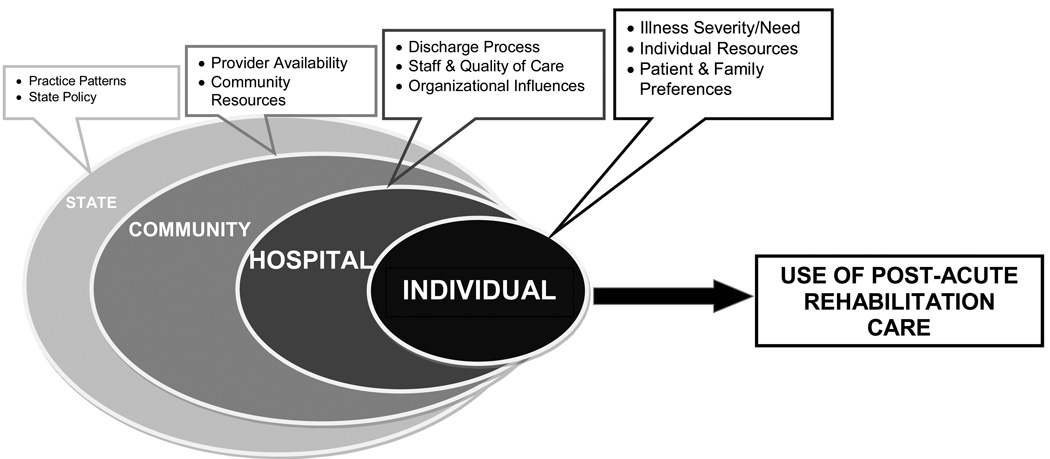
Methods: We conducted a cross-sectional analysis of 2 years (2005 and 2006) of population-based hospital discharge data from 392 hospitals in 4 states (Arizona, Florida, New Jersey, and Wisconsin). A total of 164,875 individuals who were age ≥ 45 years, admitted to the hospital for a hip or knee joint replacement, and who survived their inpatient stay were identified. Three dichotomous dependent variables were examined: 1) discharge to home versus institution (i.e., skilled nursing facility [SNF] or inpatient rehabilitation facility [IRF]), 2) discharge to home with versus without home health (HH), and 3) discharge to an SNF versus an IRF. Multilevel logistic regression analyses were conducted to identify demographic and geographic disparities in PARC use, controlling for illness severity/comorbidities, hospital characteristics, and PARC supply. Interactions among race, socioeconomic, and geographic variables were explored.
Results: Considering PARC as a continuum from more to less intensive care in regard to hours of rehabilitation per day (e.g., IRF→SNF→HH→no HH), the uninsured received less intensive care in all 3 models. Individuals receiving Medicaid and those of lower socioeconomic status received less intensive care in the HH versus no HH and SNF versus IRF models. Individuals living in rural areas received less intensive care in the institution versus home and HH versus no HH models. The effect of race was modified by insurance and by state. In most instances, minorities received less intensive care. PARC use varied by hospital.
Conclusion: Efforts to further understand the reasons behind these disparities and their effect on outcomes are needed.
Copyright © 2011 by the American College of Rheumatology.
Figures
Similar articles
-
Postacute rehabilitation care for hip fracture: who gets the most care?J Am Geriatr Soc. 2012 Oct;60(10):1929-35. doi: 10.1111/j.1532-5415.2012.04149.x. Epub 2012 Oct 4. J Am Geriatr Soc. 2012. PMID: 23036079 Free PMC article.
-
Disparities in postacute rehabilitation care for stroke: an analysis of the state inpatient databases.Arch Phys Med Rehabil. 2011 Aug;92(8):1220-9. doi: 10.1016/j.apmr.2011.03.019. Arch Phys Med Rehabil. 2011. PMID: 21807141 Free PMC article.
-
Rehabilitation following total knee replacement, total hip replacement, and hip fracture: a case-controlled comparison.J Geriatr Phys Ther. 2011 Oct-Dec;34(4):155-60. doi: 10.1519/JPT.0b013e318216db81. J Geriatr Phys Ther. 2011. PMID: 22124414
-
Association Between Patient and Facility Characteristics and Rehabilitation Outcomes After Joint Replacement Surgery in Different Rehabilitation Settings for Older Adults: A Systematic Review.J Geriatr Phys Ther. 2024 Jan-Mar 01;47(1):E1-E18. doi: 10.1519/JPT.0000000000000369. Epub 2023 Jan 4. J Geriatr Phys Ther. 2024. PMID: 36598848 Free PMC article.
-
The Effect of a Discharge Disposition Algorithm on Patient Outcomes and Satisfaction.Orthop Nurs. 2021 May-Jun 01;40(3):125-133. doi: 10.1097/NOR.0000000000000753. Orthop Nurs. 2021. PMID: 34004610 Review.
Cited by
-
Variation in Outcomes and Number of Visits Following Care Guideline Implementation: Part 2 of an Analysis of 12 355 Patients After Total Knee Arthroplasty.J Orthop Sports Phys Ther. 2023 Mar;53(3):151-158. doi: 10.2519/jospt.2022.11370. Epub 2022 Dec 12. J Orthop Sports Phys Ther. 2023. PMID: 36503269 Free PMC article. Clinical Trial.
-
Readmission Rates and Diagnoses Following Total Hip Replacement in Relation to Insurance Payer Status, Race and Ethnicity, and Income Status.J Racial Ethn Health Disparities. 2018 Dec;5(6):1202-1214. doi: 10.1007/s40615-018-0467-0. Epub 2018 Feb 12. J Racial Ethn Health Disparities. 2018. PMID: 29435896
-
Utilization of Post-Acute Care Following Distal Radius Fracture Among Medicare Beneficiaries.J Hand Surg Am. 2015 Dec;40(12):2401-9.e8. doi: 10.1016/j.jhsa.2015.08.026. Epub 2015 Oct 30. J Hand Surg Am. 2015. PMID: 26527599 Free PMC article.
-
The Disparities of Coronary Artery Bypass Grafting Surgery Outcomes by Insurance Status: A Retrospective Cohort Study, 2007-2014.World J Surg. 2018 Oct;42(10):3240-3249. doi: 10.1007/s00268-018-4631-9. World J Surg. 2018. PMID: 29691626
-
Developing quality indicators for in-patient post-acute care.BMC Geriatr. 2018 Jul 11;18(1):161. doi: 10.1186/s12877-018-0842-z. BMC Geriatr. 2018. PMID: 29996767 Free PMC article.
References
-
- Dunlop DD, Manheim LM, Song J, Sohn MW, Feinglass JM, Chang HJ, et al. Age and racial/ethnic disparities in arthritis-related hip and knee surgeries. Med Care. 2008;46(2):200–208. - PubMed
-
- Francis ML, Scaife SL, Zahnd WE, Cook EF, Schneeweiss S. Joint replacement surgeries among medicare beneficiaries in rural compared with urban areas. Arthritis Rheum. 2009;60(12):3554–3562. - PubMed
-
- Skinner J, Weinstein JN, Sporer SM, Wennberg JE. Racial, ethnic, and geographic disparities in rates of knee arthroplasty among Medicare patients. N Engl J Med. 2003;349(14):1350–1359. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
