

Accuracy of a computerized clinical decision-support system for asthma assessment and management
- PMID: 21486882
- PMCID: PMC3078658
- DOI: 10.1136/amiajnl-2010-000063
Accuracy of a computerized clinical decision-support system for asthma assessment and management
Abstract
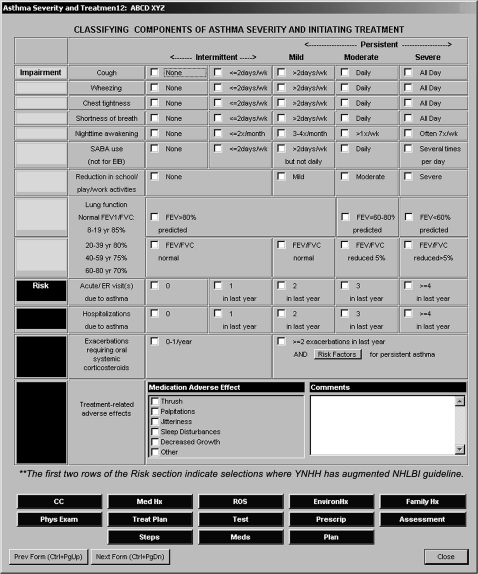
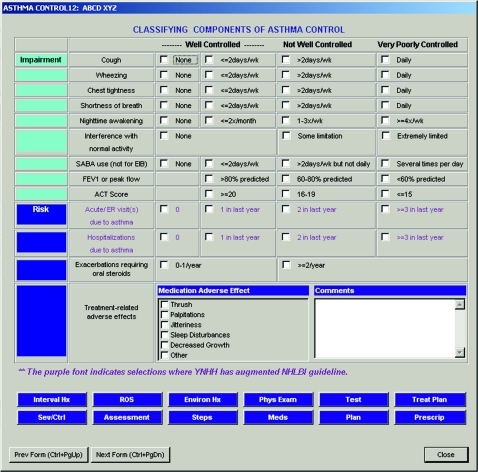
Objective: To evaluate the accuracy of a computerized clinical decision-support system (CDSS) designed to support assessment and management of pediatric asthma in a subspecialty clinic.
Design: Cohort study of all asthma visits to pediatric pulmonology from January to December, 2009.
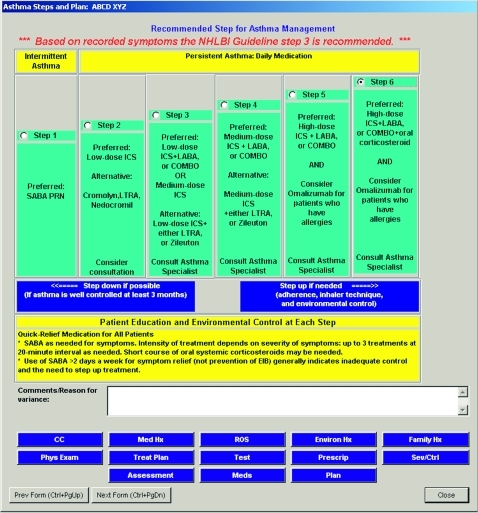
Measurements: CDSS and physician assessments of asthma severity, control, and treatment step.
Results: Both the clinician and the computerized CDSS generated assessments of asthma control in 767/1032 (74.3%) return patients, assessments of asthma severity in 100/167 (59.9%) new patients, and recommendations for treatment step in 66/167 (39.5%) new patients. Clinicians agreed with the CDSS in 543/767 (70.8%) of control assessments, 37/100 (37%) of severity assessments, and 19/66 (29%) of step recommendations. External review classified 72% of control disagreements (21% of all control assessments), 56% of severity disagreements (37% of all severity assessments), and 76% of step disagreements (54% of all step recommendations) as CDSS errors. The remaining disagreements resulted from pulmonologist error or ambiguous guidelines. Many CDSS flaws, such as attributing all 'cough' to asthma, were easily remediable. Pediatric pulmonologists failed to follow guidelines in 8% of return visits and 18% of new visits.
Limitations: The authors relied on chart notes to determine clinical reasoning. Physicians may have changed their assessments after seeing CDSS recommendations.
Conclusions: A computerized CDSS performed relatively accurately compared to clinicians for assessment of asthma control but was inaccurate for treatment. Pediatric pulmonologists failed to follow guideline-based care in a small proportion of patients.
Conflict of interest statement
Figures

References
-
- National Asthma Education Program Guidelines for the Diagnosis and Management Of Asthma. Bethesda, MD: National Heart, Lung and Blood Institute, 1991 - PubMed
-
- National Asthma Education Program Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma, 1997. http://www.nhlbi.nih.gov/guidelines/archives/epr-2/index.htm (accessed 15 Feb 2010).
-
- National Asthma Education Program Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma—Updates on Selected Topics 2002, 2002. http://www.nhlbi.nih.gov/guidelines/archives/epr-2_upd/index.htm (accessed 15 Feb 2010).
-
- National Asthma Education Program Expert Panel Report 3 (EPR 3): Guidelines for the Diagnosis and Management Of Asthma, 2007. http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm (accessed 15 Feb 2010). - PubMed
-
- Kattan M, Crain EF, Steinbach S, et al. A randomized clinical trial of clinician feedback to improve quality of care for inner-city children with asthma. Pediatrics 2006;117:e1095–103 - PubMed
