

A simulation framework for mapping risks in clinical processes: the case of in-patient transfers
- PMID: 21486883
- PMCID: PMC3078660
- DOI: 10.1136/amiajnl-2010-000075
A simulation framework for mapping risks in clinical processes: the case of in-patient transfers
Abstract
Objective: To model how individual violations in routine clinical processes cumulatively contribute to the risk of adverse events in hospital using an agent-based simulation framework.
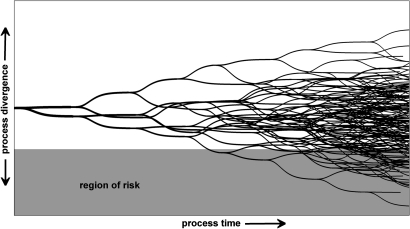
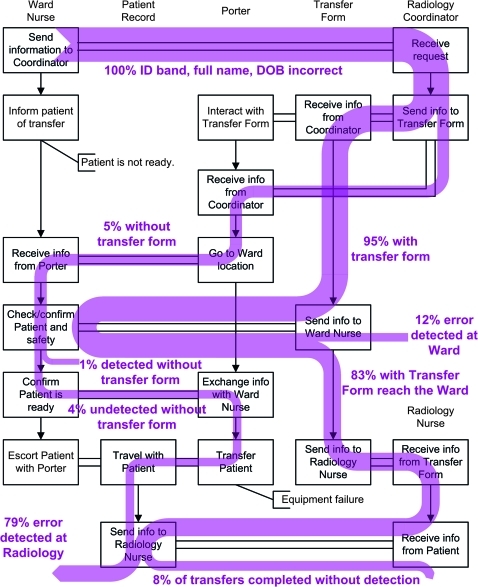
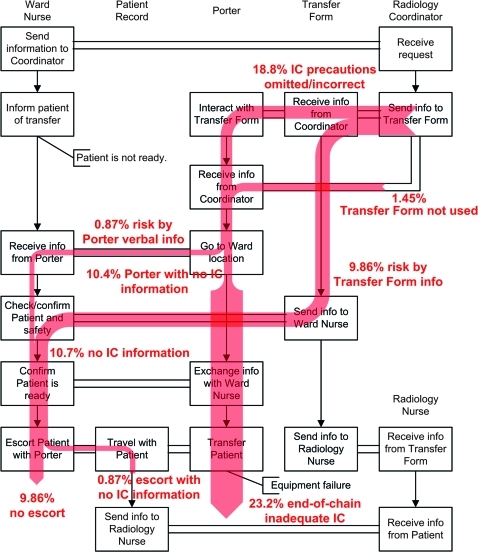
Design: An agent-based simulation was designed to model the cascade of common violations that contribute to the risk of adverse events in routine clinical processes. Clinicians and the information systems that support them were represented as a group of interacting agents using data from direct observations. The model was calibrated using data from 101 patient transfers observed in a hospital and results were validated for one of two scenarios (a misidentification scenario and an infection control scenario). Repeated simulations using the calibrated model were undertaken to create a distribution of possible process outcomes. The likelihood of end-of-chain risk is the main outcome measure, reported for each of the two scenarios.
Results: The simulations demonstrate end-of-chain risks of 8% and 24% for the misidentification and infection control scenarios, respectively. Over 95% of the simulations in both scenarios are unique, indicating that the in-patient transfer process diverges from prescribed work practices in a variety of ways.
Conclusions: The simulation allowed us to model the risk of adverse events in a clinical process, by generating the variety of possible work subject to violations, a novel prospective risk analysis method. The in-patient transfer process has a high proportion of unique trajectories, implying that risk mitigation may benefit from focusing on reducing complexity rather than augmenting the process with further rule-based protocols.
Conflict of interest statement
Figures
References
-
- Zegers M, de Bruijne MC, Wagner C, et al. Adverse events and potentially preventable deaths in Dutch hospitals: results of a retrospective patient record review study. Qual Saf Health Care 2009;18:297–302 - PubMed
-
- Runciman WB, Moller J. Iatrogenic Injury in Australia. Adelaide: Australian Patient Safety Foundation, 2001
-
- Iedema R. New approaches to researching patient safety. Soc Sci Med 2009;69:1701–4 - PubMed
