

Corticobasal degeneration: a pathologically distinct 4R tauopathy
- PMID: 21487420
- PMCID: PMC10006729
- DOI: 10.1038/nrneurol.2011.43
Corticobasal degeneration: a pathologically distinct 4R tauopathy
Abstract
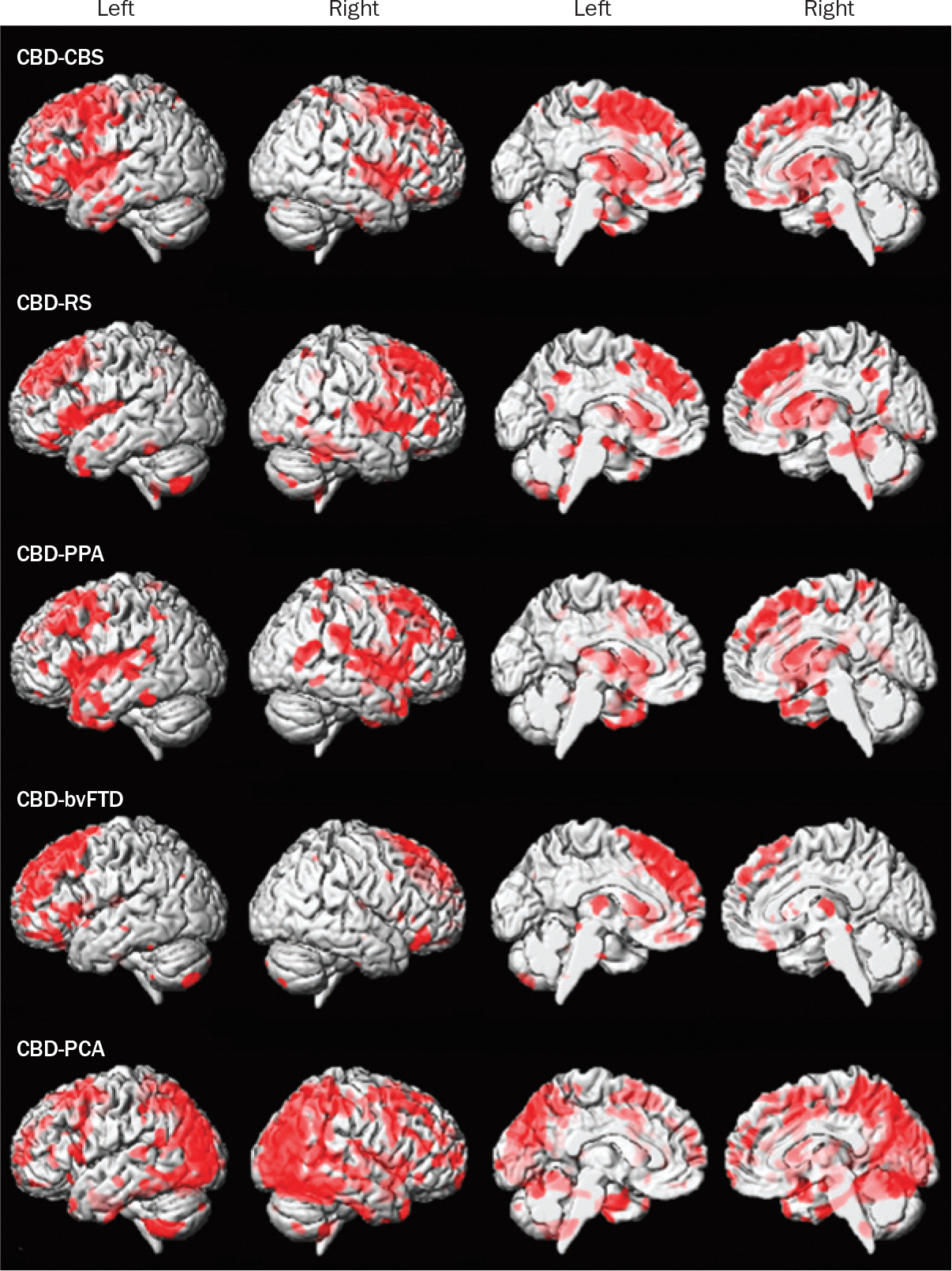
Corticobasal degeneration (CBD) is a rare, progressive neurodegenerative disorder with onset in the 5(th) to 7(th) decade of life. It is associated with heterogeneous motor, sensory, behavioral and cognitive symptoms, which make its diagnosis difficult in a living patient. The etiology of CBD is unknown; however, neuropathological and genetic evidence supports a pathogenetic role for microtubule-associated protein tau. CBD pathology is characterized by circumscribed cortical atrophy with spongiosis and ballooned neurons; the distribution of these changes dictates the patient's clinical presentation. Neuronal and glial tau pathology is extensive in gray and white matter of the cortex, basal ganglia, diencephalon and rostral brainstem. Abnormal tau accumulation within astrocytes forms pathognomonic astrocytic plaques. The classic clinical presentation, termed corticobasal syndrome (CBS), comprises asymmetric progressive rigidity and apraxia with limb dystonia and myoclonus. CBS also occurs in conjunction with other diseases, including Alzheimer disease and progressive supranuclear palsy. Moreover, the pathology of CBD is associated with clinical presentations other than CBS, including Richardson syndrome, behavioral variant frontotemporal dementia, primary progressive aphasia and posterior cortical syndrome. Progress in biomarker development to differentiate CBD from other disorders has been slow, but is essential in improving diagnosis and in development of disease-modifying therapies.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures

References
-
- Litvan I et al. Accuracy of the clinical diagnosis of corticobasal degeneration: a clinicopathologic study. Neurology 48, 119–125 (1997). - PubMed
-
- Togasaki DM & Tanner CM Epidemiologic aspects. Adv. Neurol. 82, 53–59 (2000). - PubMed
-
- Winter Y et al. Incidence of Parkinson’s disease and atypical parkinsonism: Russian population-based study. Mov. Disord. 25, 349–356 (2010). - PubMed
-
- Rebeiz JJ, Kolodny EH & Richardson EP Jr. Corticodentatonigral degeneration with neuronal achromasia. Arch. Neurol. 18, 20–33 (1968). - PubMed
-
- Gibb WR, Luthert PJ & Marsden CD Corticobasal degeneration. Brain 112, 1171–1192 (1989). - PubMed
Publication types
MeSH terms
Grants and funding
- P01-AG17216/AG/NIA NIH HHS/United States
- P50 AG016574/AG/NIA NIH HHS/United States
- R01-DC10367/DC/NIDCD NIH HHS/United States
- R01-AG37491/AG/NIA NIH HHS/United States
- P50-AG16574/AG/NIA NIH HHS/United States
- R01 AG037491/AG/NIA NIH HHS/United States
- P01 AG017216/AG/NIA NIH HHS/United States
- R21 AG038736/AG/NIA NIH HHS/United States
- R21-AG38736/AG/NIA NIH HHS/United States
- L30 AG051249/AG/NIA NIH HHS/United States
- R01 DC010367/DC/NIDCD NIH HHS/United States
- P50-NS72187/NS/NINDS NIH HHS/United States
- P50 NS072187/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
