

Relationship between functional ability in older people, immune system status, and intensity of response to CMV
- PMID: 21487706
- PMCID: PMC3312637
- DOI: 10.1007/s11357-011-9240-6
Relationship between functional ability in older people, immune system status, and intensity of response to CMV
Abstract
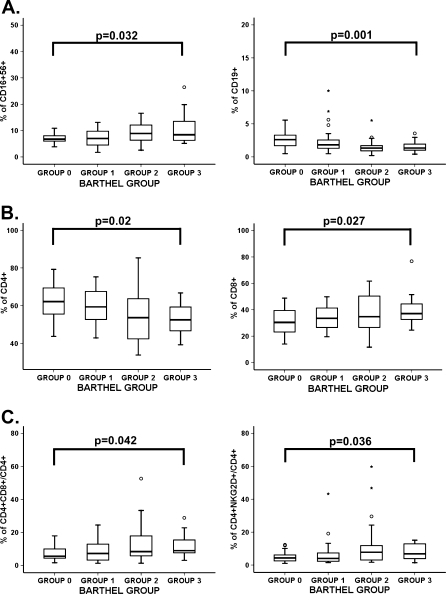
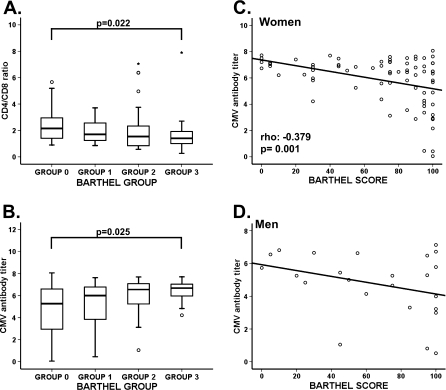
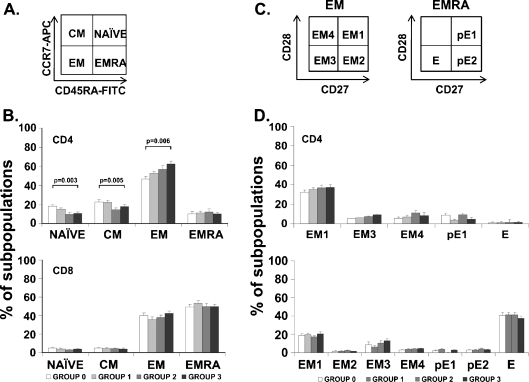
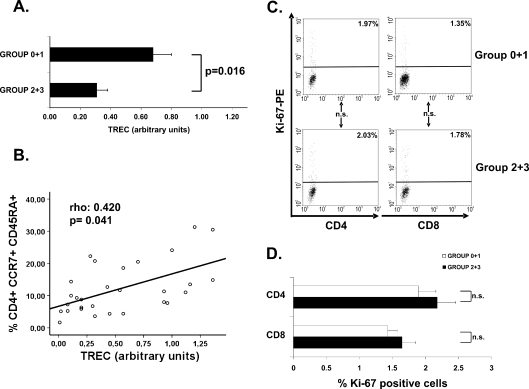
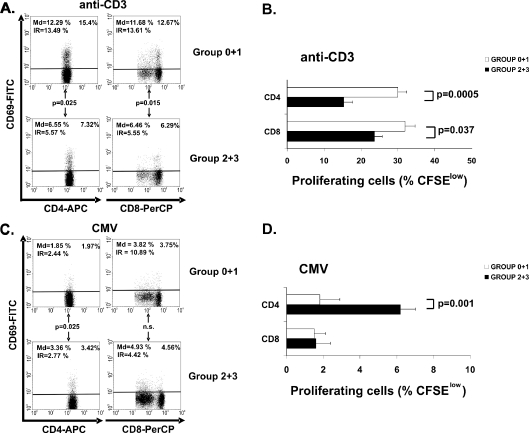
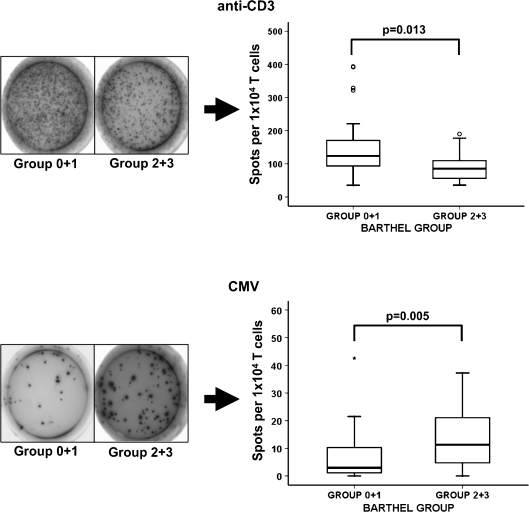
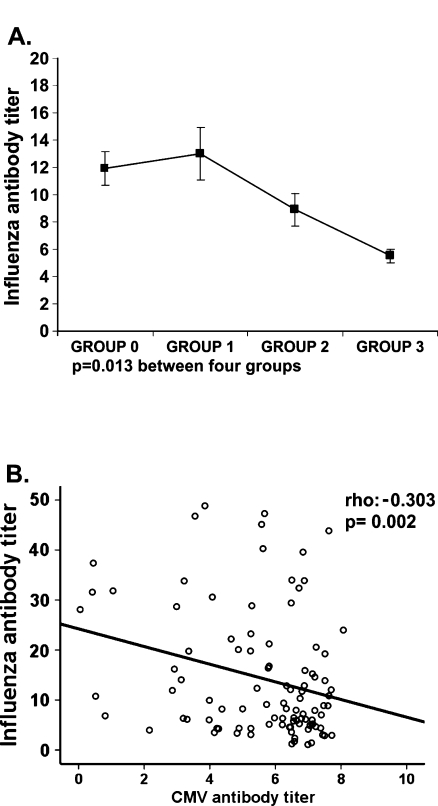
Shorter survival in the elderly has been associated with deterioration of the immune system and also with functional disability. To analyze the relationship between functional and immune impairment in older individuals, we studied 100 elderly who lived in a nursing home, were age matched, and grouped according to their functional status. We characterized cell subpopulations by flow cytometry, quantified TREC by RT-PCR, and measured the T-cell proliferation and activation response (IFN-γ by ELISPOT, CD69) against anti-CD3 and CMV. Specific antibody titers against influenza virus and CMV were determined by ELISA. Individuals with worse functional status had significantly higher levels of NK cells and fewer B cells. These poorly functioning elders also had a significantly lower proportion of CD4+ T cells, increased CD8+ T cells, and a decreased CD4/CD8 ratio. TREC levels in CD4+ T cells were significantly lower in individuals with a high disability. Lower TREC levels correlated with a lower frequency of naïve T-cell subpopulations (CD45RA+CCR7+) and higher percentages of effector cells (CD45RA-CCR7-). The functionally impaired group had lower anti-CD3 responses, but gradually increased responses against CMV. Similarly, the higher CMV titers were found in elderly with worse functional status. On the contrary, the functional response in vivo, and the titer of antibodies generated after vaccination against influenza virus, was higher in individuals with better performance status. In summary, we concluded that the functional decline of elderly individuals was clearly associated with the aging of their immune system, and the intensity of the response to CMV.
Figures
References
-
- Alonso-Arias R, Lopez-Vazquez A, Diaz-Pena R, Sampere A, Tricas L, Asensi V, Rodrigo L, Lopez-Larrea C. CD8dim and NKG2D expression defines related subsets of CD4+ T cells in HIV-infected patients with worse prognostic factors. J Acquir Immune Defic Syndr. 2009;51:390–398. doi: 10.1097/FTD.0b013e3181679015. - DOI - PubMed
-
- Appay V, Dunbar PR, Callan M, Klenerman P, Gillespie GM, Papagno L, Ogg GS, King A, Lechner F, Spina CA, Little S, Havlir DV, Richman DD, Gruener N, Pape G, Waters A, Easterbrook P, Salio M, Cerundolo V, McMichael AJ, Rowland-Jones SL. Memory CD8+ T cells vary in differentiation phenotype in different persistent virus infections. Nat Med. 2002;8:379–385. doi: 10.1038/nm0402-379. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials