

Intraoperative assessment of biliary anatomy for prevention of bile duct injury: a review of current and future patient safety interventions
- PMID: 21487883
- PMCID: PMC3142332
- DOI: 10.1007/s00464-011-1639-8
Intraoperative assessment of biliary anatomy for prevention of bile duct injury: a review of current and future patient safety interventions
Abstract
Background: Bile duct injury (BDI) is a dreaded complication of cholecystectomy, often caused by misinterpretation of biliary anatomy. To prevent BDI, techniques have been developed for intraoperative assessment of bile duct anatomy. This article reviews the evidence for the different techniques and discusses their strengths and weaknesses in terms of efficacy, ease, and cost-effectiveness.
Method: PubMed was searched from January 1980 through December 2009 for articles concerning bile duct visualization techniques for prevention of BDI during laparoscopic cholecystectomy.
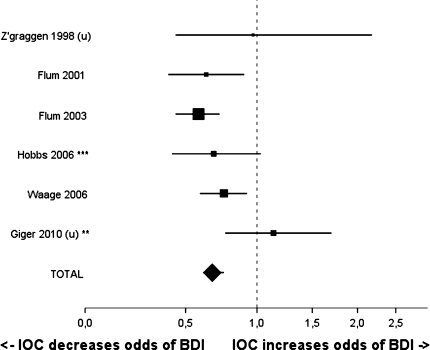
Results: Nine techniques were identified. The critical-view-of-safety approach, indirectly establishing biliary anatomy, is accepted by most guidelines and commentaries as the surgical technique of choice to minimize BDI risk. Intraoperative cholangiography is associated with lower BDI risk (OR 0.67, CI 0.61-0.75). However, it incurs extra costs, prolongs the operative procedure, and may be experienced as cumbersome. An established reliable alternative is laparoscopic ultrasound, but its longer learning curve limits widespread implementation. Easier to perform are cholecystocholangiography and dye cholangiography, but these yield poor-quality images. Light cholangiography, requiring retrograde insertion of an optical fiber into the common bile duct, is too unwieldy for routine use. Experimental techniques are passive infrared cholangiography, hyperspectral cholangiography, and near-infrared fluorescence cholangiography. The latter two are performed noninvasively and provide real-time images. Quantitative data in patients are necessary to further evaluate these techniques.
Conclusions: The critical-view-of-safety approach should be used during laparoscopic cholecystectomy. Intraoperative cholangiography or laparoscopic ultrasound is recommended to be performed routinely. Hyperspectral cholangiography and near-infrared fluorescence cholangiography are promising novel techniques to prevent BDI and thus increase patient safety.
Figures
References
-
- Graves EJ, Owings MF (1997) 1995 summary: National Hospital Discharge Survey. Adv Data 1–10 - PubMed
-
- de Reuver PR, Rauws EA, Bruno MJ, Lameris JS, Busch OR, van Gulik TM, Gouma DJ. Survival in bile duct injury patients after laparoscopic cholecystectomy: a multidisciplinary approach of gastroenterologists, radiologists, and surgeons. Surgery. 2007;142:1–9. doi: 10.1016/j.surg.2007.03.004. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
