

Clinical review: Optimal dose of continuous renal replacement therapy in acute kidney injury
- PMID: 21489322
- PMCID: PMC3219403
- DOI: 10.1186/cc9415
Clinical review: Optimal dose of continuous renal replacement therapy in acute kidney injury
Abstract
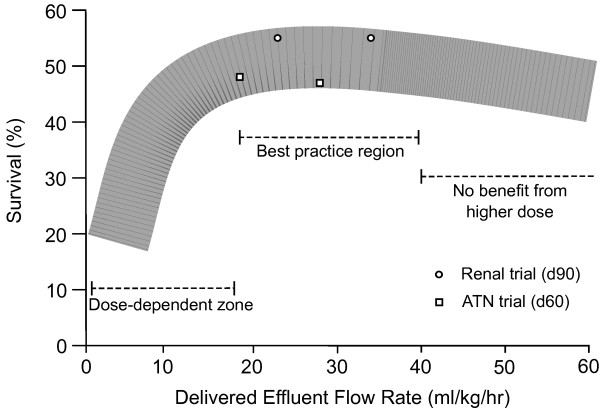
Continuous renal replacement therapy (CRRT) is the preferred treatment for acute kidney injury in intensive care units (ICUs) throughout much of the world. Despite the widespread use of CRRT, controversy and center-specific practice variation in the clinical application of CRRT continue. In particular, whereas two single-center studies have suggested survival benefit from delivery of higher-intensity CRRT to patients with acute kidney injury in the ICU, other studies have been inconsistent in their results. Now, however, two large multi-center randomized controlled trials - the Veterans Affairs/National Institutes of Health Acute Renal Failure Trial Network (ATN) study and the Randomized Evaluation of Normal versus Augmented Level (RENAL) Replacement Therapy Study - have provided level 1 evidence that effluent flow rates above 25 mL/kg per hour do not improve outcomes in patients in the ICU. In this review, we discuss the concept of dose of CRRT, its relationship with clinical outcomes, and what target optimal dose of CRRT should be pursued in light of the high-quality evidence now available.
Figures
Comment in
-
Distinction between induction and maintenance dosing in continuous renal replacement therapy.Crit Care. 2011;15(2):419; author reply 419. doi: 10.1186/cc10137. Epub 2011 Apr 26. Crit Care. 2011. PMID: 21586103 Free PMC article. No abstract available.
Similar articles
-
Continuous renal replacement therapy: recent advances and future research.Nat Rev Nephrol. 2010 Sep;6(9):521-9. doi: 10.1038/nrneph.2010.100. Epub 2010 Jul 20. Nat Rev Nephrol. 2010. PMID: 20644583 Review.
-
Prognostic Impact of Early Versus Late Initiation of Renal Replacement Therapy Based on Early Warning Algorithm in Critical Care Patients With Acute Kidney Injury.Ther Apher Dial. 2020 Aug;24(4):445-452. doi: 10.1111/1744-9987.13449. Epub 2019 Nov 29. Ther Apher Dial. 2020. PMID: 31661596
-
Estimating the impact of renal replacement therapy choice on outcome in severe acute renal failure.Clin Nephrol. 2005 May;63(5):335-45. doi: 10.5414/cnp63335. Clin Nephrol. 2005. PMID: 15909592
-
Do we know the optimal dose for renal replacement therapy in the intensive care unit?Kidney Int. 2006 Oct;70(7):1202-4. doi: 10.1038/sj.ki.5001827. Kidney Int. 2006. PMID: 16988729
-
Dose in continuous renal replacement therapy.Gac Med Mex. 2018;154(Supp 1):S40-S47. doi: 10.24875/GMM.M18000069. Gac Med Mex. 2018. PMID: 30074025 Review.
Cited by
-
Renal replacement therapy: a practical update.Can J Anaesth. 2019 May;66(5):593-604. doi: 10.1007/s12630-019-01306-x. Epub 2019 Feb 6. Can J Anaesth. 2019. PMID: 30725343 Review. English.
-
Application of continuous renal replacement therapy for acute kidney injury in elderly patients.Int J Clin Exp Med. 2015 Jun 15;8(6):9973-8. eCollection 2015. Int J Clin Exp Med. 2015. PMID: 26309685 Free PMC article.
-
Knowledge, attitude, practice, needs, and implementation status of intensive care unit staff toward continuous renal replacement therapy: a survey of 66 hospitals in central and South China.BMC Nurs. 2024 Apr 26;23(1):281. doi: 10.1186/s12912-024-01953-6. BMC Nurs. 2024. PMID: 38671501 Free PMC article.
-
The effect of a loading dose of meropenem on outcomes of patients with sepsis treated by continuous renal replacement: study protocol for a randomized controlled trial.Trials. 2022 Apr 12;23(1):294. doi: 10.1186/s13063-022-06264-2. Trials. 2022. PMID: 35413886 Free PMC article.
-
Beta-lactam dosing in critically ill patients with septic shock and continuous renal replacement therapy.Crit Care. 2014 Jun 23;18(3):227. doi: 10.1186/cc13938. Crit Care. 2014. PMID: 25042938 Free PMC article. Review.
References
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C. Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–818. doi: 10.1001/jama.294.7.813. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
