

doi: 10.4061/2011/378041.
Multimodality imaging in the evaluation of cardiovascular manifestations of malignancy
Affiliations
- PMID: 21490697
- PMCID: PMC3066556
- DOI: 10.4061/2011/378041
Item in Clipboard
Multimodality imaging in the evaluation of cardiovascular manifestations of malignancy
Cardiol Res Pract.
.
Abstract
Up to one third of the population will die as a direct result of cancer. Accurate and timely diagnosis of disease often requires multiple different approaches including the use of modern imaging techniques. Prompt recognition of adverse consequences of some anti-cancer therapies also requires a knowledge of the optimum imaging strategy for the problem at hand. The purpose of this article is to review not only some of the commoner cardiovascular manifestations of malignancy but also to discuss the strengths, weaknesses and appropriate use of cardiovascular imaging modalities.
Figures
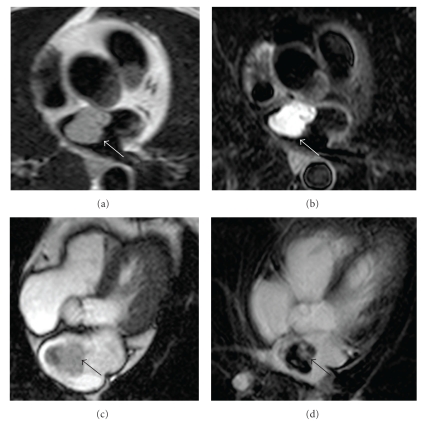
Left atrial myxoma. A lobulated mass is situated in the left atrium adjacent to the interatrial septum (a). On T2-weighted images, the mass appears uniformly high signal ((b), white arrow). Note that the mass is less well appreciated on bright blood cine imaging ((c), black arrow) and could be overlooked if it were smaller. Late gadolinium enhancement images (d) demonstrate patchy uptake of contrast within the mass (black arrow). The location and imaging characteristics are fairly typical for myxoma.

Fibroma. An ovoid mass partially obstructs the right ventricular outflow tract ((a)–(f), asterisk). The mass is of intermediate intensity on T1-weighted imaging ((a) and (b)) and low signal on T2-weighted imaging (c). This combination of findings would make malignancy relatively unlikely since many neoplasms have a relatively high water content and thus are high signal on T2 sequences. Dramatic contrast uptake is, however, evident on the postgadolinium images ((e) and (f)). Dense fibrous tumors may behave in this way, and the diagnosis of fibroma was later confirmed.

Teratoma. A well-circumscribed solid mass is present adjacent to the right atrial appendage ((b), (c), (f) asterisk). Foci of low attenuation are identified within it on noncontrast axial MDCT ((a), white arrows). Similar areas can be seen on the T1-weighted image ((d), white arrow) and show signal “dropout” with a fat-suppressed sequence ((e), white arrow). The presence of fat in a mixed density mediastinal lesion raised the possibility of teratoma, and this diagnosis was confirmed at pathology.

Bronchogenic carcinoma. A large mass (asterisk) is shown in axial ((a) and (b)) and coronal ((c) and (d)) planes. On T1-weighted images the mass demonstrates significant near-uniform enhancement after gadolinium contrast ((a) and (c) before contrast; (b) and (d) after contrast). The mass infiltrates posterior to the carina ((a), white arrow) and occludes the left main bronchus ((c) and (d), white arrow). The left main pulmonary artery is severely attenuated ((c), black arrow).
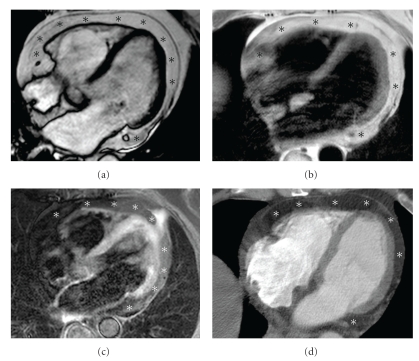
Epicardial fat. Echocardiography raised concerns about excessive soft tissue anterior to the right ventricle in this patient on long-term steroids. Bright blood cine (a) and T1-weighted images (b) show circumferential high signal around the heart (asterisks). The appearances suggest an unusual amount of pericardial fat, and this was confirmed on fat-suppressed CMR (c) where there is evidence of signal drop out from the fatty region (asterisks—compare with (b)). MDCT is also very sensitive for fat which it displays as low-density regions of negative Hounsfield attenuation ((d), asterisks). Excessive mediastinal lipomatosis is not uncommon in patients taking steroid preparations.

Mitral annular calcification (MAC). A classic “pseudotumour” MAC is seen in older patients, often with a history of diabetes or hypertension. It presents as focal mass-like lesions most frequently adjacent to the lateral mitral annulus ((a) and (b), white arrow). In this example the signal characteristics on CMR are typically being low signal on T1-weighted images (a) and T2-weighted images (b). Its relation to the posterior mitral annulus is well appreciated on the short axis bright-blood cine view ((c), white arrow). Noncontrast MDCT excludes any residual diagnosis about the diagnosis—the mass is of very high attenuation consistent with calcium ((d), white arrow).

Thrombus. A coronal maximum intensity projection image from a contrast MDCT study demonstrates multiple pulmonary emboli ((a), white arrows). On the same study the possibility of a right atrial mass was raised ((b), white arrow), although it was uncertain whether this was real or simply an appearance due to incomplete mixing of opacified SVC blood with unopacified IVC blood. Cine CMR demonstrates that the mass is clearly real ((c), black arrow). Further characterization by CMR demonstrates that the mass is low signal on T1 weighted images ((d), white arrow) and remains low signal following gadolinium administration ((e), white arrow). The appearances and clinical presentation were entirely consistent with right atrial thrombus. The mass disappeared with subsequent anticoagulation.

Echo signs of tamponade. Diastolic inversion of the right atrial (RA) free wall is an early sign of raised intrapericardial pressure ((a) and (b)), white arrow—note collapse/inversion of the RA free wall in early diastole (b) as the intrapericardial pressure exceeds the RA pressure. Right ventricular diastolic inversion is a later but more specific sign of tamponade ((c) and (d)) asterisks outline the RV free wall—the RV shows diastolic collapse (d) due to the adjacent effusion (PE). Note also the relative enlargement of the left ventricle (LV) in this case; a result of chemotherapy-related cardiomyopathy. Doppler techniques are often very helpful in establishing the diagnosis of tamponade—transtricuspid flow variability of greater than 33% on a beat-to-beat basis ((e), asterisks represent peak transtricuspid flow for each recorded beat) is suggestive of tamponade. M-mode Doppler has a very high sampling (frame) rate compared to standard B-mode Doppler and is therefore useful for timing the motion of the RV free wall with respect to the cardiac cycle ((f), horizontal white arrows indicate the RV free wall; as would be expected this moves in normally during systole but is slow to move outwards in early-to-mid diastole (black asterisks)—in fact full outward excursion only occurs late in diastole (dotted short arrow) aided by the filling from atrial contraction (dotted long arrow indicates P wave on ECG, i.e., atrial systole)).
Similar articles
-
Clinical Practice Guideline: Evaluation of the Neck Mass in Adults.Otolaryngol Head Neck Surg. 2017 Sep;157(2_suppl):S1-S30. doi: 10.1177/0194599817722550. Otolaryngol Head Neck Surg. 2017. PMID: 28891406
-
Multimodality imaging evaluation of Chagas disease: an expert consensus of Brazilian Cardiovascular Imaging Department (DIC) and the European Association of Cardiovascular Imaging (EACVI).Eur Heart J Cardiovasc Imaging. 2018 Apr 1;19(4):459-460n. doi: 10.1093/ehjci/jex154. Eur Heart J Cardiovasc Imaging. 2018. PMID: 29029074
-
Sepsis Care Pathway 2019.Qatar Med J. 2019 Nov 7;2019(2):4. doi: 10.5339/qmj.2019.qccc.4. eCollection 2019. Qatar Med J. 2019. PMID: 31763206 Free PMC article.
-
Role of multimodality imaging in the diagnosis and management of cardiomyopathies.Arch Cardiovasc Dis. 2019 Oct;112(10):615-629. doi: 10.1016/j.acvd.2019.07.004. Epub 2019 Oct 10. Arch Cardiovasc Dis. 2019. PMID: 31607558 Review.
-
Differentiating Rheumatoid and Psoriatic Arthritis of the Hand: Multimodality Imaging Characteristics.Radiographics. 2020 Sep-Oct;40(5):1339-1354. doi: 10.1148/rg.2020200029. Epub 2020 Jul 31. Radiographics. 2020. PMID: 32735474 Review.
Cited by
-
Direct Left Ventricular Metastasis Reduction: 3D-Echo Monitoring For Management of Clinical Case.J Cardiovasc Echogr. 2013 Jul-Sep;23(3):84-87. doi: 10.4103/2211-4122.123955. J Cardiovasc Echogr. 2013. PMID: 28465891 Free PMC article.
References
-
- Klein GJ, Thirion JP. Cardiovascular imaging to quantify the evolution of cardiac diseases in clinical development. Biomarkers. 2005;10(supplement 1):S1–S9. - PubMed
-
- Del Castillo SV, Aguilar Torres R, Paré Bardera JC. Update on cardiac imaging techniques: echocardiography, cardiac magnetic resonance, and multidetector computed tomography. Revista Espanola de Cardiologia. 2009;62(supplement 1):129–150. - PubMed
-
- Douglas PS, Khandheria B, Stainback RF, et al. ACCF/ASE/ACEP/ASNC/SCAI/SCCT/SCMR 2007 appropriateness criteria for transthoracic and transesophageal echocardiography. Journal of the American College of Cardiology. 2007;50(2):187–204. - PubMed
-
- Rao G, Sajnani N, Kusnetzky LL, Main ML. Appropriate use of transthoracic echocardiography. American Journal of Cardiology. 2010;105(11):1640–1642. - PubMed
-
- Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. Journal of the American College of Cardiology. 2006;48(3):e1–e148. - PubMed
LinkOut - more resources
Full Text Sources