

The optimal volume of 0.2% ropivacaine required for an ultrasound-guided stellate ganglion block
- PMID: 21490819
- PMCID: PMC3071481
- DOI: 10.4097/kjae.2011.60.3.179
The optimal volume of 0.2% ropivacaine required for an ultrasound-guided stellate ganglion block
Abstract
Background: This study was performed to find the optimal volume of local anesthetics needed for a successful ultrasound-guided stellate ganglion block (SGB) to treat head and neck pathology.
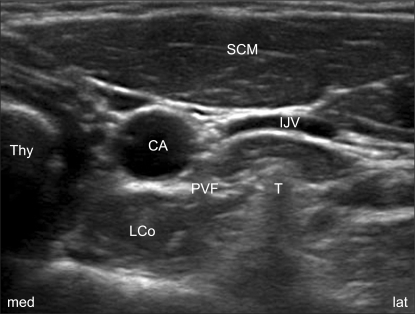
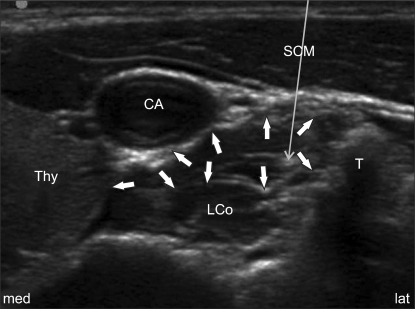
Methods: Fifteen female and fourteen male sensory-neural hearing loss patients received 4 times SGBs with 0.2% ropivacaine in volumes of 6, 4, 3 and 2 ml at 1 to 3 day intervals. Using the transverse short-axis view of the neck that showed Chassaignac's tubercle at the C6 level, a 25-gauge, and 4 cm needle was inserted via the lateral paracarotid approach with out-of-plane targeting between the prevertebral fascia and the ventral surface of longus colli muscle (subfascial injection). A successful block was confirmed with the onset of ptosis (Horner's syndrome).
Results: There were no significant statistical differences between the presence of Horner's syndrome and the volume of local anesthetics given. However, Horner's syndrome was present in all trials for the 4 ml and 6 ml groups. Six (20.7%) and three out (10.4%) of twenty-nine trials in the 2 ml and 3 ml groups, respectively, failed to elicit Horner's syndrome. The duration of action was significantly different in the 2 ml group compared to that of the 6 ml group, but there was no significant difference between the other groups, including the 4 ml vs. 6 ml groups. The side effects were not different between the groups.
Conclusions: This data suggests that the optimal volume of 0.2% ropivacaine for ultrasound-guided SGB to treat the head and neck pathology in daily practice is 4 ml.
Keywords: Local anesthetics; Stellate ganglion block; Ultrasound; Volume.
Figures
References
-
- Song SO, Jo YW. Effects of the volume of local anesthetic used in stellate ganglion block on the elevation of skin temperature of ipsilateral upper extremity. Korean J Anesthesiol. 1999;37:233–239.
-
- Cho YW, Song SO, Jang JH. Effect of stellate ganglion block using 0.2% ropivacaine. J Korean Pain Soc. 2000;13:182–186.
-
- Chang JH, Song SO. Minimal concentration of lidocaine for a diagnostic stellate ganglion block. Korean J Anesthesiol. 2001;41:165–170.
-
- Song SO, Suh YH. Changes of plasma lidocaine concentrations after stellate ganglion block according to volume-changes of 1% lidocaine. J Korean Pain Soc. 2001;14:26–31.
-
- Lee HK, Chung SY, Yang SK, Lee HJ, Suh YS, Kim C. Minimal volume of local anesthetic for successful stellate ganglion block. J Korean Pain Soc. 1995;8:60–64.
LinkOut - more resources
Full Text Sources
Medical
