

Management of Duodenal Adenomas Involving the Ampulla of Vater - A Warning against Limited Resection
- PMID: 21490846
- PMCID: PMC3075174
- DOI: 10.1159/000119321
Management of Duodenal Adenomas Involving the Ampulla of Vater - A Warning against Limited Resection
Abstract
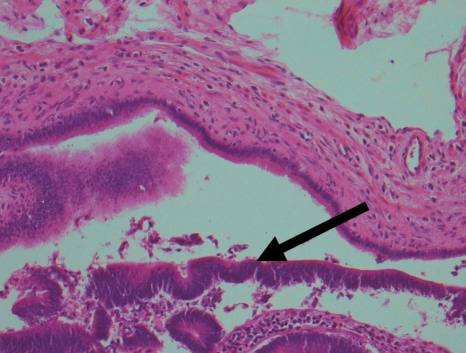
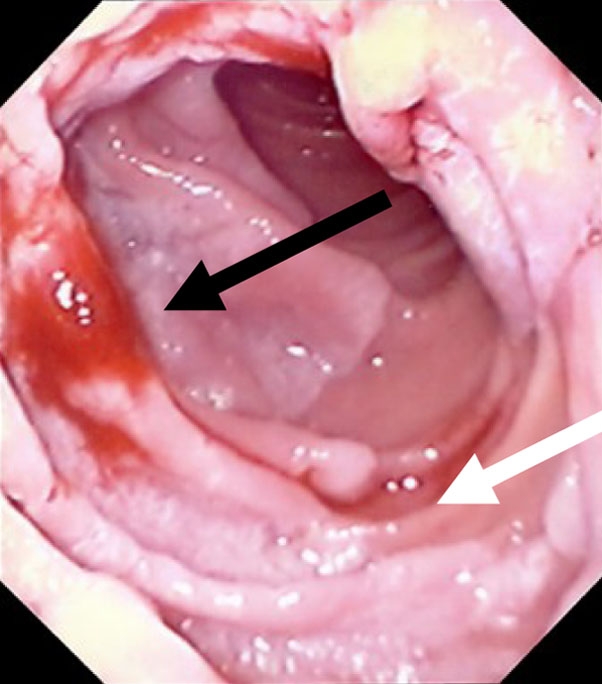
Duodenal adenomas are uncommon, however, when present a proportion have dysplasia associated with the adenoma and therefore require treatment. The options range from less invasive endoscopic treatments to a pancreaticoduodenectomy. This case report describes two patients with adenomas involving the ampulla of Vater. One patient had familial adenomatous polyposis, the other was a renal transplant patient with a large adenoma. Both patients' adenomas contained high-grade dysplasia. Both patients underwent a pancreaticoduodenectomy. Histology of both specimens demonstrated that the adenoma had migrated up the bile duct for at least 7 mm, and the pancreatic duct for 8 mm in one patient. Limited resection of ampullary adenomas may leave residual adenomatous tissue in the bile duct with the risk of recurrent adenomatous disease and malignant transformation.
Keywords: Ampullary adenoma/carcinoma; Duodenal adenoma/carcinoma; High-grade dysplasia; Management; Surgery.
Figures



Similar articles
-
Endoscopic ultrasound evaluation in the surgical treatment of duodenal and peri-ampullary adenomas.World J Gastroenterol. 2013 Jan 28;19(4):511-5. doi: 10.3748/wjg.v19.i4.511. World J Gastroenterol. 2013. PMID: 23382629 Free PMC article.
-
Long-term outcome after ampullectomy for ampullary lesions associated with familial adenomatous polyposis.Dis Colon Rectum. 2005 Dec;48(12):2192-6. doi: 10.1007/s10350-005-0187-5. Dis Colon Rectum. 2005. PMID: 16228827
-
Endoscopy and EUS are key for effective surveillance and management of duodenal adenomas in familial adenomatous polyposis.Gastrointest Endosc. 2015 Apr;81(4):960-6. doi: 10.1016/j.gie.2014.08.029. Epub 2014 Oct 24. Gastrointest Endosc. 2015. PMID: 25440680
-
Ampullary tumors: endoscopic versus operative management.Surg Innov. 2004 Dec;11(4):255-63. doi: 10.1177/155335060401100409. Surg Innov. 2004. PMID: 15756395 Review.
-
Adenoma of the papilla and ampulla--premalignant lesions?Langenbecks Arch Surg. 2001 Apr;386(3):172-5. doi: 10.1007/s004230100234. Langenbecks Arch Surg. 2001. PMID: 11382317 Review.
Cited by
-
Review of the investigation and surgical management of resectable ampullary adenocarcinoma.HPB (Oxford). 2013 Nov;15(11):829-38. doi: 10.1111/hpb.12038. Epub 2013 Jan 10. HPB (Oxford). 2013. PMID: 23458317 Free PMC article.
References
-
- Jepsen JM, Persson M, Jakobsen NO, Christiansen T, Skoubo-Kristensen E, Funch-Jensen P, et al. Prospective study of prevalence and endoscopic and histopathologic characteristics of duodenal polyps in patients submitted to upper endoscopy. Scand J Gastroenterol. 1994;29:483–487. - PubMed
-
- Charton JP, Deinert K, Schumacher B, Neuhaus H. Endoscopic resection for neoplastic diseases of the papilla of Vater. J Hepatobiliary Pancreat Surg. 2004;11:245–251. - PubMed
-
- Lienert A, Bagshaw P. Treatment of duodenal adenomas with endoscopic argon plasma coagulation. ANZ J Surg. 2007;77:371–373. - PubMed
-
- Park SW, Song SY, Chung JB, Lee SK, Moon YM, Kang JK, et al. Endoscopic snare resection for tumors of the ampulla of Vater. Yonsei Med J. 2000;41:213–218. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
