

ERCP in total situs viscerum inversus
- PMID: 21490849
- PMCID: PMC3075177
- DOI: 10.1159/000119713
ERCP in total situs viscerum inversus
Abstract
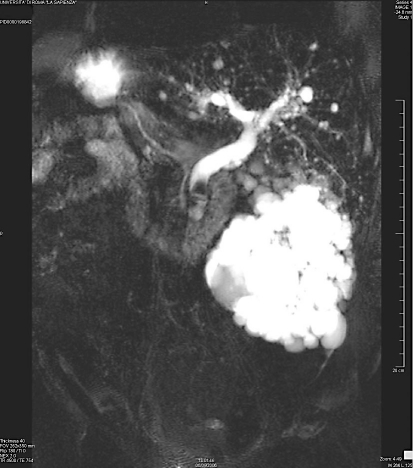
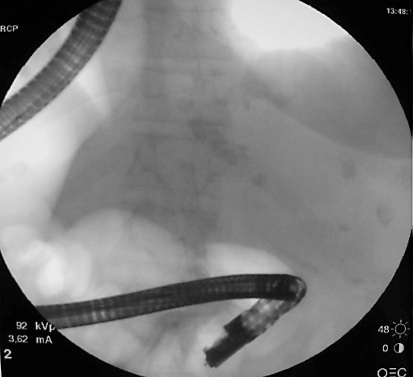
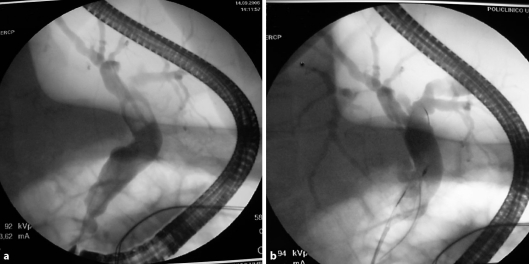
A 69-year-old cholecystectomized female with known total situs viscerum inversus presented recurrent colicky pain in the left upper abdominal quadrant and jaundice. Laboratory parameters showed increased neutrophils and coniugated bilirubin of 5.53 mg/dl. US and MRCP confirmed total situs viscerum inversus and a dilatation of the intra- and extrahepatic ducts with a peripapillary 13 mm stone. ERCP, sphincterotomy and successful common bile duct stone extraction were performed in the conventional way. ERCP was carried out successfully despite situs inversus maintaining the patient in the prone position with the endoscopist on the right side of the table. Some authors have reported similar cases in whom ERCP was performed in other positions, while this report shows that an experienced endoscopist can achieve the same results in the conventional way as it is possible when anatomical changes, Billroth II or Roux-en-Y, or different positions of the patient, supine or on the left side, are present.
Keywords: Bile duct stones; ERCP; Endoscopic sphincterotomy; Total situs viscerum inversus.
Figures
References
-
- Gastrointestinal: situs inversus viscerum. J Gastroenterol Hepatol. 2002;17:1329. - PubMed
-
- Therapeutic Endoscopy . Color Atlas of Operative Techniques for the Gastrointestinal Tract. Berlin: Thieme; 2005. p. 88.
-
- Pathak KA, Khanna R, Khanna N. Situs inversus with cholelithiasis. J Postgrad Med. 1995;41:45–46. - PubMed
-
- Terruzzi V, Radaelli F, Meucci G, Minoli G. Is the supine position as safe and effective as the prone position for endoscopic retrograde cholangiopancreatography? A prospective randomized study. Endoscopy. 2005;37:1211–1214. - PubMed
-
- Hintze RE, Adler A, Veltzke W, Abou-Rebyeh H. Endoscopic access to the papilla of Vater for endoscopic retrograde cholangiopancreatography in patients with Billroth II and Roux-en-Y gastrojejunostomy. Endoscopy. 1997;29:69–73. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
