

Bilateral Morgagni Hernia: Primary Repair without a Mesh
- PMID: 21490893
- PMCID: PMC3075148
- DOI: 10.1159/000142371
Bilateral Morgagni Hernia: Primary Repair without a Mesh
Abstract
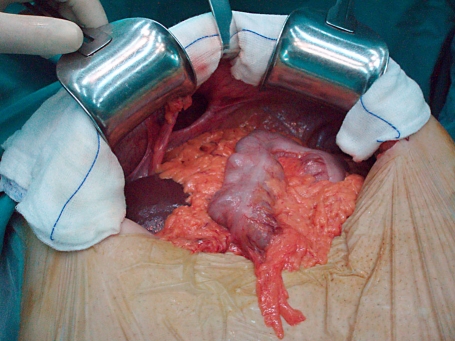
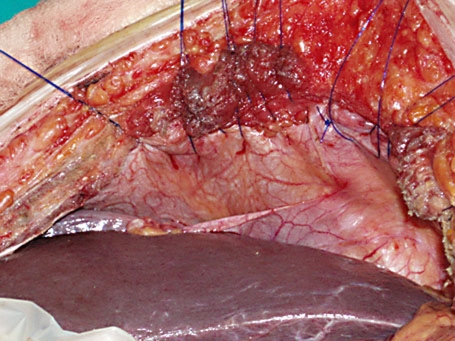
We present a case of bilateral Morgagni hernia in a 68-year-old male with an intermittent history of progressive onset of breath shortness and occasional cardiac arrhythmias. Diagnosis was made by clinical examination and the findings in a plain chest radiograph and was confirmed by computed tomography scan. The patient was operated electively and subjected to a transabdominal approach. A bilateral subcostal incision revealed a large right side anterior diaphragmatic defect with a hernia containing the ascending colon, the majority of the transverse colon and a huge amount of omentum. Also a second smaller defect was found on the left side with no hernia inside. After large bowel and omentum had been taken down to the peritoneal cavity, both defects were primarily closed using interrupted nylon sutures without the use of a mesh. The patient recovered very well, had an uneventful postoperative course and was released on the 5th postoperative day. 15-month follow-up failed to reveal any signs of recurrence.
Keywords: Bilateral Morgagni hernia; Mesh; Transabdominal approach.
Figures


References
-
- Harrington SW. Clinical manifestations and surgical treatment of congenital types of diaphragmatic hernia. Rev Gastroenterol. 1951;18:243–256. - PubMed
-
- Comer TP, Clagett OT. Surgical treatment of hernia of the foramen of Morgagni. J Thorac Cardiovasc Surg. 1966;52:461–468. - PubMed
-
- Kilic D, Nadir A, Doner E, Kavukcu S, Akal M, Ozdemir N, Akay H, Okten I. Transthoracic approach in surgical management of Morgagni hernia. Eur J Cardiothorac Surg. 2001;20:1016–1019. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
