

Skeletonized coronary arteries: pathophysiological and clinical aspects of vascular calcification
- PMID: 21490939
- PMCID: PMC3072737
- DOI: 10.2147/VHRM.S16328
Skeletonized coronary arteries: pathophysiological and clinical aspects of vascular calcification
Abstract
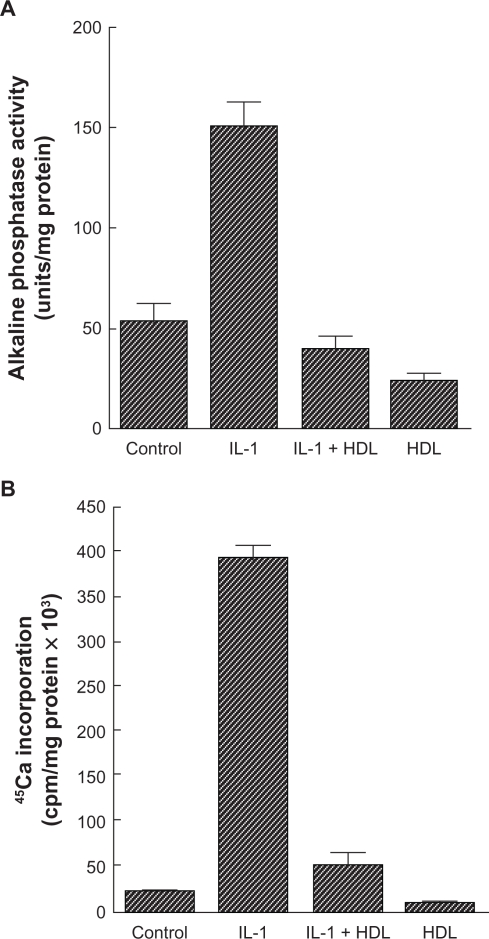
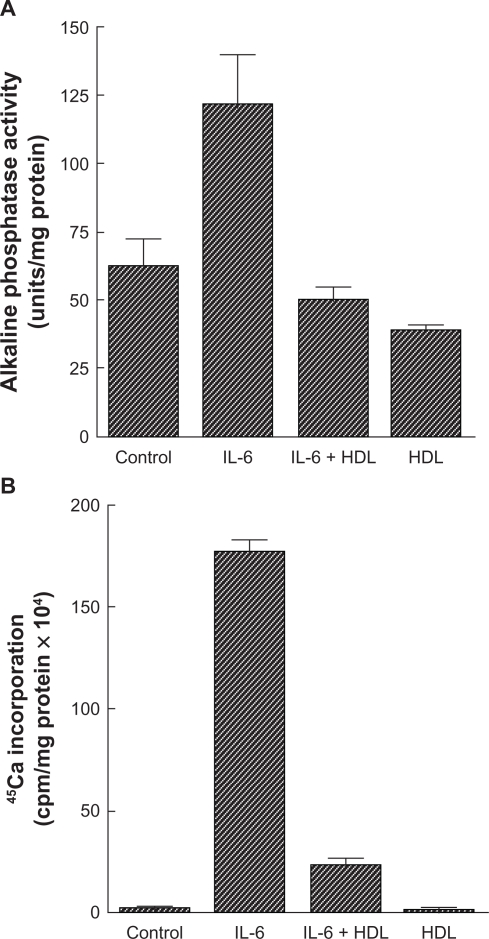
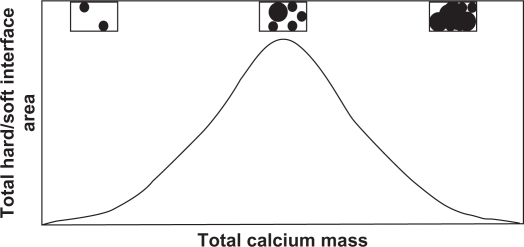
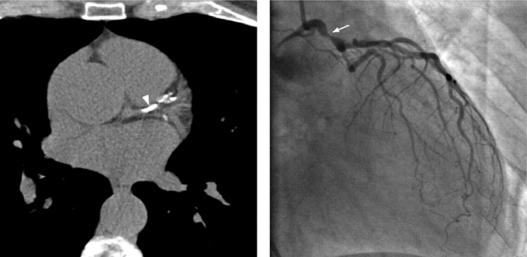
The role of calcification in coronary artery disease is gaining importance, both in research studies and in clinical application. Calcified plaque has long been considered to be the most important atherosclerotic plaque within the arterial tree and frequently presents a challenge for percutaneous intervention. Current investigations have shown that plaque calcification has a dynamic course that is closely related to the magnitude of vascular inflammation. Numerous inflammatory factors synthesized during the early stages of atherosclerosis induce the expression and activation of osteoblast-like cells localized in the arterial wall that produce calcium. There is no doubt that the role of these factors in calcification associated with coronary artery disease could be a crucial strategic point in prevention and treatment. A number of diagnostic imaging methods have been developed in recent years, but their performance needs to be improved. In this context, we undertook an update on coronary calcification, focusing on physiopathology, clinical implications, and imaging techniques.
Keywords: atherosclerotic plaques; vascular calcification; vascular smooth muscle cells.
Figures


References
-
- Frink RJ, Achor RW, Brown AL, Jr, Kincaid OW, Brandenburg RO. Significance of calcification of the coronary arteries. Am J Cardiol. 1970;26:241–247. - PubMed
-
- Moses JW, Carlier S, Moussa I. Lesion preparation prior to stenting. Rev Cardiovasc Med. 2004;5(Suppl 2):S16–S21. - PubMed
-
- Abedin M, Tintut Y, Demer LL. Vascular calcification: Mechanisms and clinical ramifications. Arterioscler Thromb Vasc Biol. 2004;24:1161–1170. - PubMed
-
- Dhore CR, Cleutjens JP, Lutgens E, et al. Differential expression of bone matrix regulatory proteins in human atherosclerotic plaques. Arterioscler Thromb Vasc Biol. 2001;21:1998–2003. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
