

Preliminary outcomes 1 year after laparoscopic sleeve gastrectomy based on Bariatric Analysis and Reporting Outcome System (BAROS)
- PMID: 21491136
- PMCID: PMC3217142
- DOI: 10.1007/s11695-011-0403-4
Preliminary outcomes 1 year after laparoscopic sleeve gastrectomy based on Bariatric Analysis and Reporting Outcome System (BAROS)
Abstract
Background: The aim of this study was to assess outcomes of laparoscopic sleeve gastrectomy (LSG) as a stand-alone bariatric operation according to the Bariatric Analysis and Reporting Outcome System (BAROS).
Methods: Out of 112 patients included and operated on initially, 84 patients (F/M, 63:21) were followed up for 14-56 months (mean 22 ± 6.75). Patients lost to follow-up did not attend scheduled follow-up visits or they have withdrawn their consent. Mean age was 39 years (range 17-67; SD ± 12.09) with mean initial BMI 44.62 kg/m(2) (range 29.39-82.8; SD ± 8.17). Statistical significance was established at the p < 0.05 level.
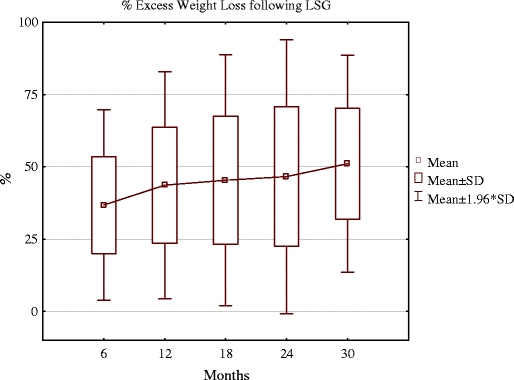
Results: Mean operative time was 61 min (30-140 min) with mean hospital stay of 1.37 days (0-4; SD ± 0.77). Excellent global BAROS outcome was achieved in 13% of patients, very good in 30%, good in 34.5%, fair 9.5% and failure in 13% patients 12 months after surgery. Females achieved significantly better outcomes than males with the mean 46.5% of excess weight loss (EWL) versus 35.3% of EWL at 12 months (p = 0.02). The mean percentage of excess weight loss (%EWL) was 43.6% at 12 months and 46.6% at 24 months. Major surgical complication rate was 7.1%; minor surgical complication rate 8.3%. There was one conversion (1.2%) due to the massive bleeding. Comorbidities improved or resolved in numerous patients: arterial hypertension in 62%, diabetes mellitus in 68.3%, respectively.
Conclusions: Presented LSG series shows that the LSG as a stand-alone procedure provides acceptable %EWL and good global BAROS outcomes. It significantly improves comorbidities as well.
Figures
References
-
- Karlsson J, Sjöström L, Sullivan M. Swedish obese subjects (SOS)—an intervention study of obesity. Two-year-follow-up of health-related quality of life (HRQL) and eating behavior after gastric surgery for severe obesity. Int J Obes Relat Metab Disord. 1998;22:113–26. doi: 10.1038/sj.ijo.0800553. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
