

Non-pharmacological interventions for perceptual disorders following stroke and other adult-acquired, non-progressive brain injury
- PMID: 21491397
- PMCID: PMC6465074
- DOI: 10.1002/14651858.CD007039.pub2
Non-pharmacological interventions for perceptual disorders following stroke and other adult-acquired, non-progressive brain injury
Update in
-
Interventions for perceptual disorders following stroke.Cochrane Database Syst Rev. 2022 Nov 3;11(11):CD007039. doi: 10.1002/14651858.CD007039.pub3. Cochrane Database Syst Rev. 2022. PMID: 36326118 Free PMC article.
Abstract
Background: Stroke and other adult-acquired brain injury may impair perception leading to distress and increased dependence on others. Perceptual rehabilitation includes functional training, sensory stimulation, strategy training and task repetition.
Objectives: To examine the evidence for improvement in activities of daily living (ADL) six months post randomisation for active intervention versus placebo or no treatment.
Search strategy: We searched the trials registers of the Cochrane Stroke Group and the Cochrane Infectious Diseases Group (May 2009) but not the Injuries Group, the Cochrane Central Register of Controlled Trials (The Cochrane Library 2009, Issue 3), MEDLINE (1950 to August 2009), EMBASE (1980 to August 2009), CINAHL (1982 to August 2009), PsycINFO (1974 to August 2009), REHABDATA and PsycBITE (May to June 2009). We also searched trials and research registers, handsearched journals, searched reference lists and contacted authors.
Selection criteria: Randomised controlled trials of adult stroke or acquired brain injury. Our definition of perception excluded visual field deficits, neglect/inattention and apraxia.
Data collection and analysis: One review author assessed titles, abstracts and keywords for eligibility. At least two review authors independently extracted data. We requested unclear or missing information from corresponding authors.
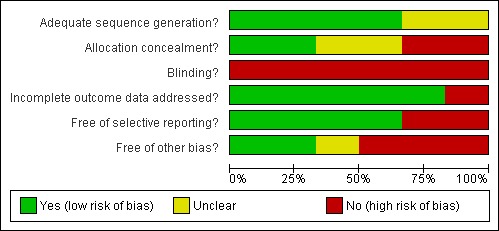
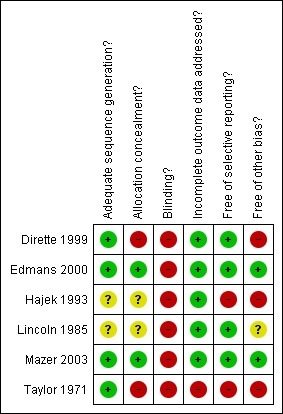
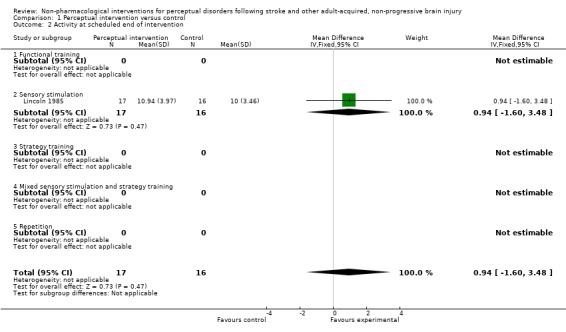
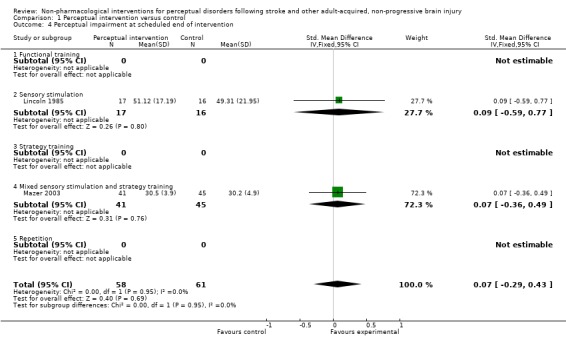
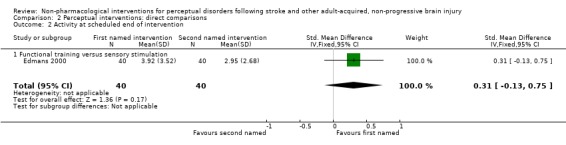
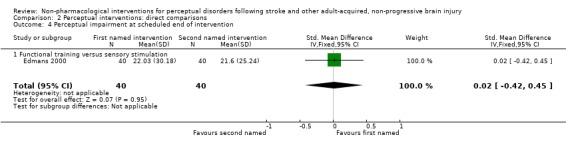
Main results: We included six single-site trials in rehabilitation settings, involving 338 participants. Four trials included people with only stroke. All studies provided sensory stimulation, sometimes with another intervention. Sensory stimulation typically involved practising tasks that required visuo-perceptual processing with occupational therapist assistance. Repetition was never used and only one study included functional training. No trials provided data on longer term improvement in ADL scores. Only three trials provided any data suitable for analysis. Two of these trials compared active to placebo intervention. There was no evidence of a difference in ADL scores at the scheduled end of intervention: mean difference (95% confidence interval (CI)) was 0.9 (-1.6 to 3.5) points on a self-care ADL scale in one study and odds ratio (95% CI) was 1.3 (0.56 to 3.1) for passing a driving test in the other, both in favour of active intervention. The trial that compared two active interventions did not find evidence of difference in any of the review outcomes.
Authors' conclusions: There is insufficient evidence to support or refute the view that perceptual interventions are effective. Future studies should be sufficiently large, include a standard care comparison and measure longer term functional outcomes. People with impaired perception problems should continue to receive neurorehabilitation according to clinical guidelines.
Conflict of interest statement
None known
Figures
Comment in
-
[Is a specific rehabilitation worthwhile in perceptual disorders?].Dtsch Med Wochenschr. 2011 Aug;136(34-35):1710. doi: 10.1055/s-0031-1286351. Epub 2011 Aug 29. Dtsch Med Wochenschr. 2011. PMID: 21877301 German. No abstract available.
References
References to studies included in this review
-
- Dirette DK, Hinojosa J, Carnevale GJ. Comparison of remedial and compensatory interventions for adults with acquired brain injuries. Journal of Head Trauma Rehabilitation 1999;14(6):595‐601. - PubMed
-
- Edmans JA, Webster J, Lincoln N. A comparison of two approaches in the treatment of perceptual problems after stroke. Clinical Rehabilitation 2000;14:230‐43. - PubMed
-
- Hajek VE, Kates MH, Donnelly R, McGree S. The effect of visuo‐spatial training in patients with right hemisphere stroke. Canadian Journal of Rehabilitation 1993;6(3):175‐86.
-
- Lincoln NB, Whiting SE, Cockburn J, Bhavnani G. An evaluation of perceptual retraining. International Rehabilitation Medicine 1985;7:99‐101. - PubMed
-
- Mazer B, Sofer S, Korner‐Bitensky N, Gelinas I, Hanley J, Wood‐Dauphinee S. Effectiveness of a visual attention retraining program on the driving performance of clients with stroke. Archives of Physical Medicine and Rehabilitation 2003;84:541‐50. - PubMed
References to studies excluded from this review
-
- Beschin N, Cocchini G, Della Sala S. Effect of optokinetic stimulation, prism adaptation and tens on anosognosia for motor deficits. In: Proceedings of the The Stroke Association 10th Scientific Conference. 2005.
-
- Carter LT, Howard BE, O'Neil WA. Effectiveness of cognitive skill remediation in acute stroke patients. American Journal of Occupational Therapy 1983;37:320‐6. - PubMed
-
- Connor BB, Wing AM, Humphreys GW, Bracewell RM, Harvey DA. Errorless learning using haptic guidance: research in cognitive rehabilitation following stroke. Proceedings of the 4th International Conference on Disability, Virtual Reality and Associated Technologies. 2002:77‐83.
-
- Flynn A. Investigation into whether psychology led cognitive rehabilitation of attentional and visio‐spatial skills improves performance in these areas beyond spontaneous recovery. National Research Register2001, issue 1:https://portal.nihr.ac.uk/Profiles/NRR.aspx?Publication_ID=N0280012930 (accessed 21 January 2011).
-
- Gordon WA, Hibbard MR, Egelko S, Diller L, Shaver MS, Lieberman A, et al. Perceptual remediation in patients with right brain damage: a comprehensive program. Archives of Physical Medicine and Rehabilitation 1985;66:353‐9. - PubMed
References to studies awaiting assessment
-
- Kang SH, Kim D‐K, Seo KM, Choi KM, Yoo JY, Sung SY, et al. A computerised visual perception rehabilitation programme with interactive computer interface using motion tracking technology ‐ a randomised controlled, single blinded, pilot clinical trial study. Clinical Rehabilitation 2009;23:434‐44. - PubMed
-
- Leer WB. . . Block Design Training with Stroke Patients: A Study on the Effects of Cognitive Retraining on Improving Certain Activities of Daily Living Skills. Michigan, USA: Michigan State University, 1984.
-
- Matz K, Teuschl Y, Eckhardt R, Herbst A, Dachenhausen A, Brainin M. Cognitive training in patients with first lacunar stroke ‐ a randomized pilot trial for the prevention of post‐stroke cognitive decline. Cerebrovascular Diseases 2007;23 Suppl 2:42.
References to ongoing studies
-
- Ongoing study Starting date of trial not provided. Contact author for more information.
Additional references
-
- Beaumont J, Davidoff J. In: Crawford JR, Parker DM, McKinlay WW editor(s). A handbook of neuropsychological assessment. Hove: Lawrence Earlbaum Associates, 1992.
-
- Cicerone KD, Dahlberg C, Malec JF, Langenbahn DM, Felicetti T, Kneipp S, et al. Evidence‐based cognitive rehabilitation:updated review of the literature from 1998‐2002. Archives of Physical Medicine and Rehabilitation 2005;86:1681‐92. - PubMed
-
- Hospital Episode Statistics. Department of Health, UK 2000‐2001.
-
- Donnan GA, Fisher M, Macleod M, Davis SM. Stroke. Lancet 2008;371:1612‐23. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical