

Ultra-radical (extensive) surgery versus standard surgery for the primary cytoreduction of advanced epithelial ovarian cancer
- PMID: 21491400
- PMCID: PMC4028614
- DOI: 10.1002/14651858.CD007697.pub2
Ultra-radical (extensive) surgery versus standard surgery for the primary cytoreduction of advanced epithelial ovarian cancer
Update in
-
Ultra-radical (extensive) surgery versus standard surgery for the primary cytoreduction of advanced epithelial ovarian cancer.Cochrane Database Syst Rev. 2022 Aug 30;8(8):CD007697. doi: 10.1002/14651858.CD007697.pub3. Cochrane Database Syst Rev. 2022. PMID: 36041232 Free PMC article.
Abstract
Background: Ovarian cancer is the sixth most common cancer among women and the leading cause of death in women with gynaecological malignancies. Opinions differ regarding the role of ultra-radical (extensive) cytoreductive surgery in ovarian cancer treatment.
Objectives: To evaluate the effectiveness and morbidity associated with ultra-radical/extensive surgery in the management of advanced stage ovarian cancer.
Search strategy: We searched the Cochrane Gynaecological Cancer Group Trials Register, Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2010, Issue 4), MEDLINE and EMBASE (up to November 2010). We also searched registers of clinical trials, abstracts of scientific meetings, reference lists of included studies and contacted experts in the field.
Selection criteria: Randomised controlled trials (RCTs) or non-randomised studies, analysed using multivariate methods, that compared ultra-radical/extensive and standard surgery in adult women with advanced primary epithelial ovarian cancer.
Data collection and analysis: Two review authors independently assessed whether potentially relevant studies met the inclusion criteria, abstracted data and assessed the risk of bias. One non-randomised study was identified so no meta-analyses were performed.
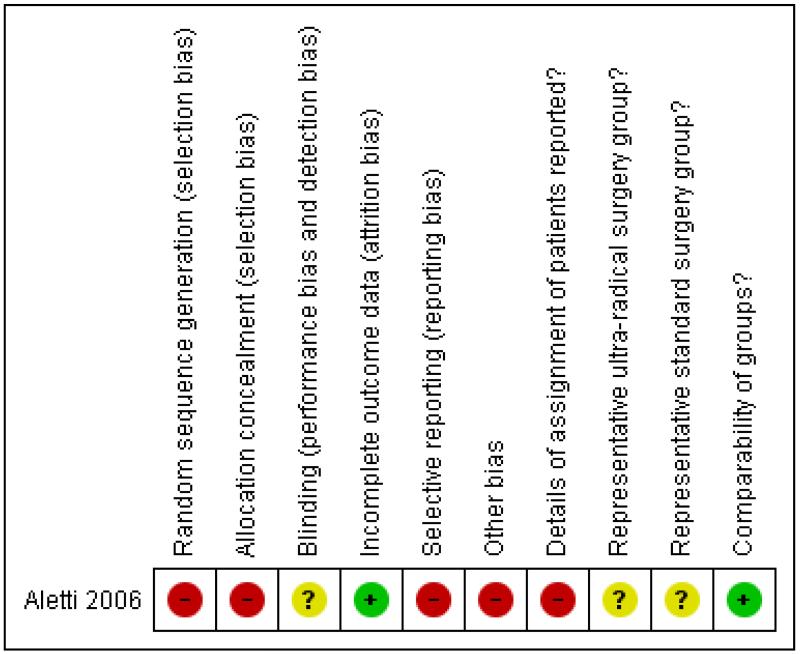
Main results: One non-randomised study met our inclusion criteria. It analysed retrospective data for 194 women with stage IIIC advanced epithelial ovarian cancer who underwent either ultra-radical (extensive) or standard surgery and reported disease specific overall survival and perioperative mortality. Multivariate analysis, adjusted for prognostic factors, identified better disease specific survival among women receiving ultra-radical surgery, although this was not statistically significant (Hazard ratio (HR) = 0.64, 95% confidence interval (CI): 0.40 to 1.04). In a subset of 144 women with carcinomatosis, those who underwent ultra-radical surgery had significantly better disease specific survival than women who underwent standard surgery (adjusted HR = 0.64, 95% CI 0.41 to 0.98). Progression-free survival and quality of life (QoL) were not reported and adverse events were incompletely documented. The study was at high risk of bias.
Authors' conclusions: We found only low quality evidence comparing ultra-radical and standard surgery in women with advanced ovarian cancer and carcinomatosis. The evidence suggested that ultra-radical surgery may result in better survival. It was unclear whether there were any differences in progression-free survival, QoL and morbidity between the two groups. The cost-effectiveness of this intervention has not been investigated. We are, therefore, unable to reach definite conclusions about the relative benefits and adverse effects of the two types of surgery.In order to determine the role of ultra-radical surgery in the management of advanced stage ovarian cancer, a sufficiently powered randomised controlled trial comparing ultra-radical and standard surgery or well-designed non-randomised studies would be required.
Figures
References
-
- Aletti GD, Dowdy SC, Gostout BS, Jones MB, Stanhope CR, Wilson TO, et al. Aggressive surgical effort and improved survival in advanced-stage ovarian cancer. Obstetrics and Gynecology. 2006;107(1):77–85. [published data only] - PubMed
References to studies excluded from this review
-
- Aletti GD, Dowdy SC, Podratz KC, Cliby WA. Surgical treatment of diaphragm disease correlates with improved survival in optimally debulked advanced stage ovarian cancer. Gynecologic Oncology. 2006;100(2):283–7. [published data only] - PubMed
-
- Aletti GD, Podratz KC, Jones MB, Cliby WA. Role of rectosigmoidectomy and stripping of pelvic peritoneum in outcomes of patients with advanced ovarian cancer. Journal of the American College of Surgeons. 2006;203(4):521–6. [published data only] - PubMed
-
- Aletti GD, Dowdy SC, Gostout BS, Jones MB, Stanhope RC, Wilson TO, et al. Quality Improvement in the Surgical Approach to Advanced Ovarian Cancer: The Mayo Clinic Experience. Journal of the American College of Surgeons. 2009;208:614–20. [published data only] - PubMed
-
- Aletti GD, Podratz KC, Moriarity JP, Cliby WA, Long KH. Aggressive and complex surgery for advanced ovarian cancer: An economic analysis. Gynecologic Oncology. 2009;112:16–21. [published data only] - PubMed
-
- Bertelsen K. Tumor reduction surgery and long-term survival in advanced ovarian cancer: a DACOVA study. Gynecologic Oncology. 1990;38(2):203–9. [published data only] - PubMed
Additional references
-
- Bristow RE, del Carmen MG, Kaufman HS, Montz FJ. Radical oophrectomy with primary stapled colorectal anastomosis for resection of locally advanced epithelial ovarian cancer. Journal of the American College of Surgeons. 2003;197:565–74. - PubMed
-
- Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: A meta-analysis. Journal of Clinical Oncology. 2002;20:1248–59. - PubMed
-
- Chen SS, Bochner R. Assessment of morbidity and mortality in primary cytoreductive surgery for advanced ovarian carcinoma. Gynecologic Oncology. 1985;20:190–95. - PubMed
-
- Covens AL. A critique of surgical cytoreduction in advanced ovarian cancer. Gynecologic Oncology. 2000;78:269–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous