

Workplace interventions for neck pain in workers
- PMID: 21491405
- PMCID: PMC6485986
- DOI: 10.1002/14651858.CD008160.pub2
Workplace interventions for neck pain in workers
Abstract
Background: Musculoskeletal disorders are the most common cause of disability in many industrial countries. Recurrent and chronic pain accounts for a substantial portion of workers' absenteeism. Neck pain seems to be more prominent in the general population than previously known.
Objectives: To determine the effectiveness of workplace interventions (WIs) in adult workers with neck pain.
Search strategy: We searched: CENTRAL (The Cochrane Library 2009, issue 3), and MEDLINE, EMBASE, CINAHL, PsycINFO, ISI Web of Science, OTseeker, PEDro to July 2009, with no language limitations;screened reference lists; and contacted experts in the field.
Selection criteria: We included randomised controlled trials (RCT), in which at least 50% of the participants had neck pain at baseline and received interventions conducted at the workplace.
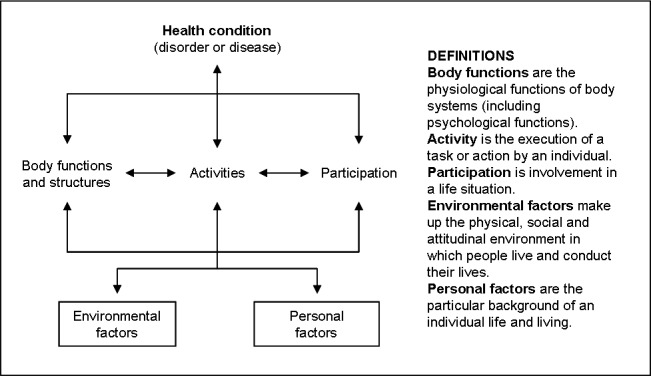
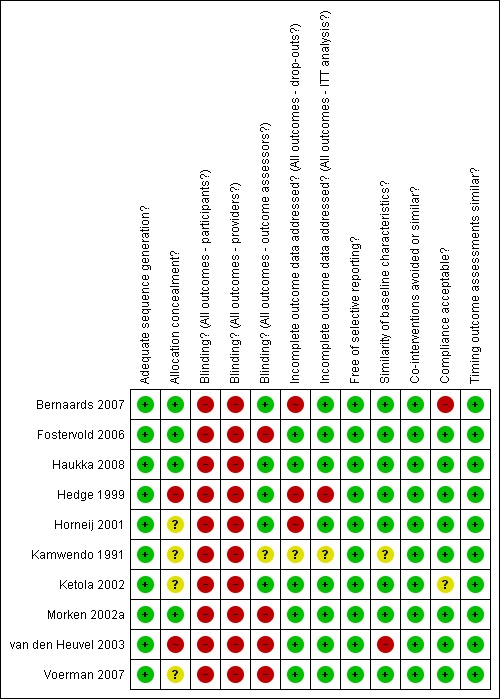
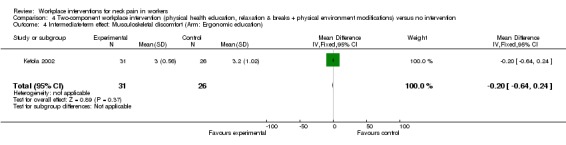
Data collection and analysis: Two review authors independently extracted data and assessed risk of bias. Authors were contacted for missing information. Since the interventions varied to a large extend, International Classification of Functioning, Disability and Health (ICF) terminology was used to classify the intervention components. This heterogeneity restricted pooling of data to only one meta-analysis of two studies.
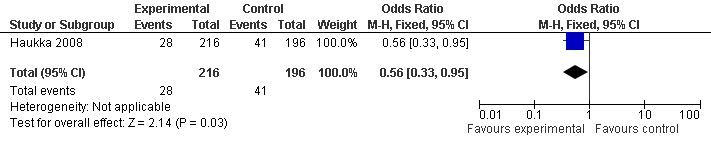
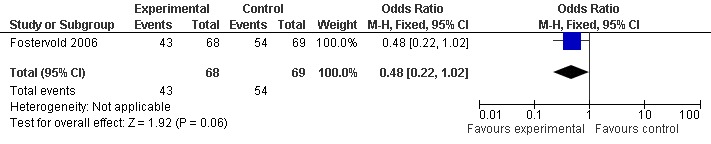
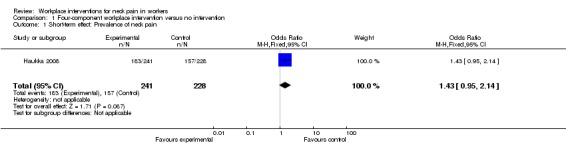
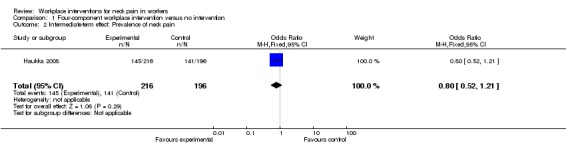
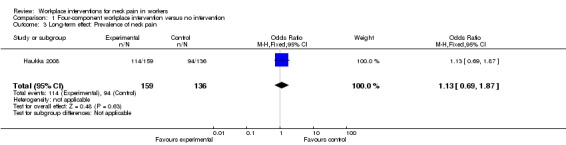
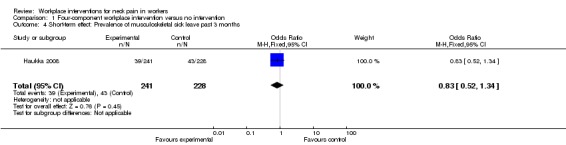
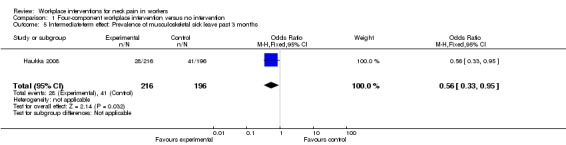
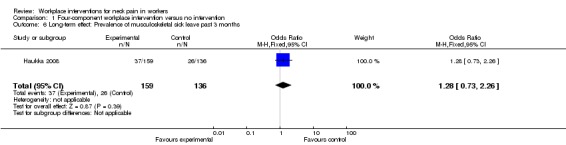
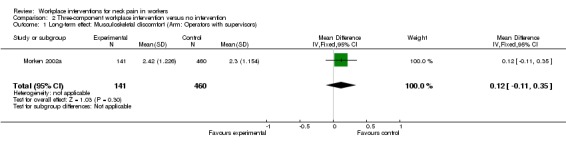
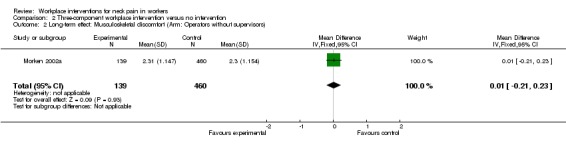
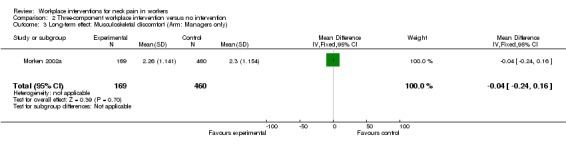
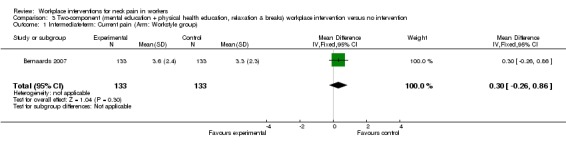
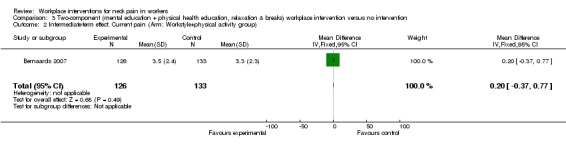
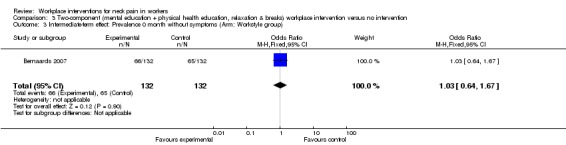
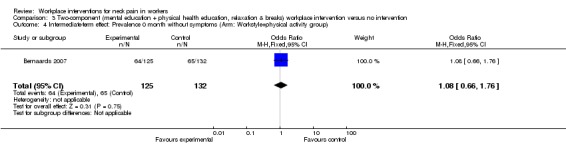
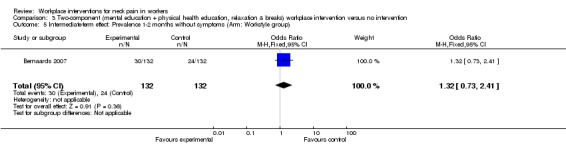
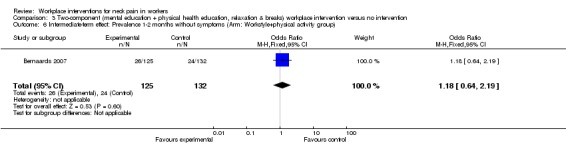
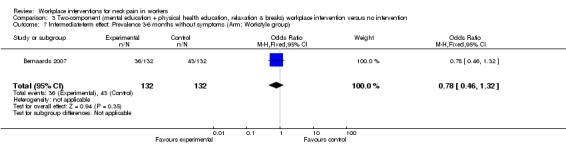
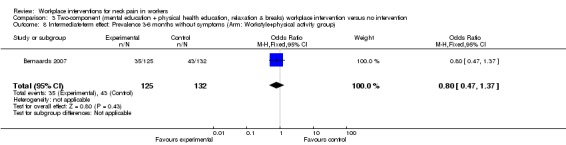
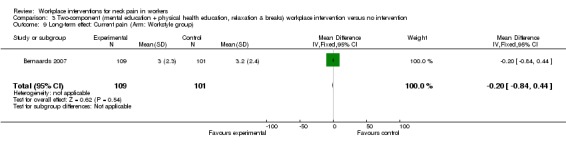
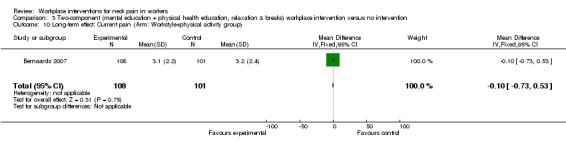
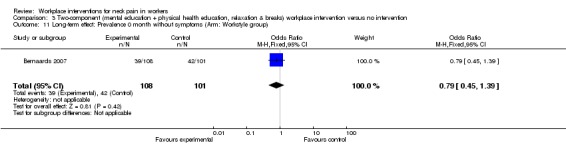
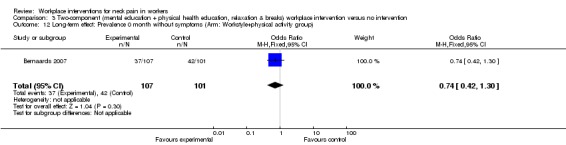
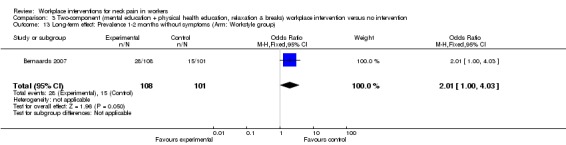
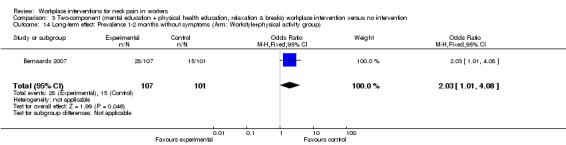
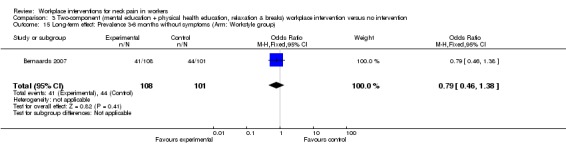
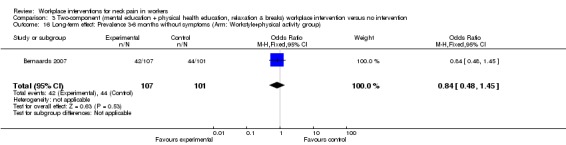
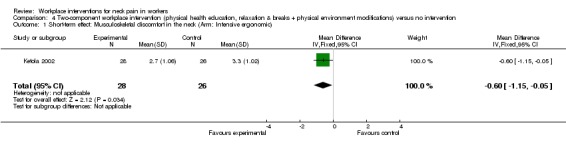
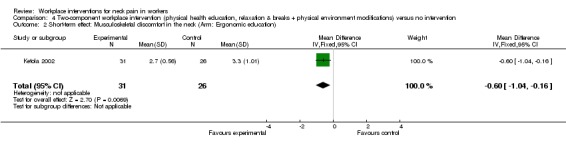
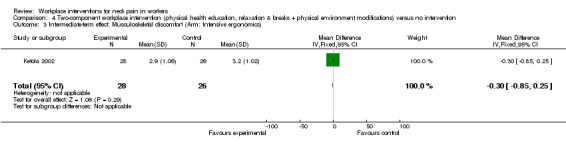
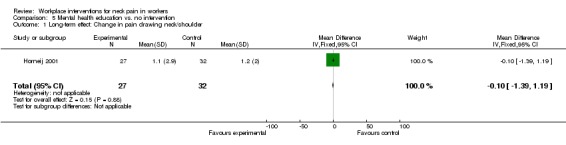
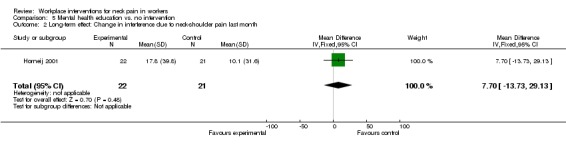
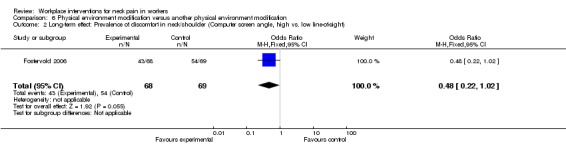
Main results: We identified 1995 references and included10 RCTs (2745 workers). Two studies were assessed with low risk of bias. Most trials (N = 8) examined office workers. Few workers were sick-listed. Thus, WIs were seldom designed to improve return-to-work. Overall, there was low quality evidence that showed no significant differences between WIs and no intervention for pain prevalence or severity. If present, significant results in favour of WIs were not sustained across follow-up times. There was moderate quality evidence (1 study, 415 workers) that a four-component WI was significantly more effective in reducing sick leave in the intermediate-term (OR 0.56, 95% CI 0.33 to 0.95), but not in the short- (OR 0.83, 95% CI 0.52 to 1.34) or long-term (OR 1.28, 95% CI 0.73 to 2.26). These findings might be because only a small proportion of the workers were sick-listed.
Authors' conclusions: Overall, this review found low quality evidence that neither supported nor refuted the benefits of any specific WI for pain relief and moderate quality evidence that a multiple-component intervention reduced sickness absence in the intermediate-term, which was not sustained over time. Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. There is an urgent need for high quality RCTs with well designed WIs.
Conflict of interest statement
None known.
Figures



Update of
References
References to studies included in this review
-
- Bernaards CM, Ariens GAM, Knol DL, Hildebrandt VH. The effectiveness of a work style intervention and a lifestyle physical activity intervention on the recovery from neck and upper limb symptoms in computer workers. Pain 2007;132:142‐53. - PubMed
-
- Fostervold KI, Aarås A, Lie I. Work with visual display units: Long‐term health effects of high and downward line‐of‐sight in ordinary office environments. International Journal of Industrial Ergonomics 2006;36:331‐43.
-
- Haukka E, Leino‐Arjas P, Viikari‐Juntura E, Takala EP, Malmivaara A, Hopsu L, et al. A randomised controlled trial on whether a participatory ergonomics intervention could prevent musculoskeletal disorders. Occupational and Environmental Medicine 2008;65:849‐56. - PubMed
-
- Hedge A, Morimoto S, McCrobie D. Effects of keyboard tray geometry on upper body posture and comfort. Ergonomics 1999;42(10):1333‐49. - PubMed
-
- Horneij E, Hernborg B, Jensen I, Ekdahl C. No significant differences between intervention programmes on neck, shoulder and low back pain: A prospective randomized study among home‐care personnel. J Rehabil Med 2001;33:170‐6. - PubMed
References to studies excluded from this review
-
- Aarås A, Ro O, Thorsen M. Can a More Neutral Position of the Forearm When Operating a Computer Mouse Reduce the Pain Level for Visial Display Unit Operators? A Prospective Epidemiological Intervention Study. International Journal of Human‐Computer Interaction 1999;11(2):79‐94.
-
- Arnetz BB, Sjögren B, Rydēhn B, Meisel R. Early workplace intervention for employees with musculoskeletal ‐related absenteeism: A prospective controlled intervention study. Journal of occupational and environmental medicine 2003;45(5):499‐506. - PubMed
-
- Borchgrevink GE, Kaasa AA, McDonagh D, Stiles TC, Haraldseth O, Lereim I. Acute treatment of whiplash neck sprain injuries. Spine 1998;23(1):25‐31. - PubMed
-
- Brisson C, Montreuil S, Punnett L. Effects of an ergonomic training program on workers with video display units. Scandinavian Journal of Work Environment and Health 1999;25(3):255‐63. - PubMed
-
- Bultmann U, Sherson D, Olsen J, Hansen CL, Lund T, Kilsgaard J. Coordinated and tailored work rehabilitation: a randomized controlled trial with economic evaluation undertaken with workers on sick leave due to musculoskeletal disorders. Journal of Occupational Rehabilitation 2009;19(1):81‐93. - PubMed
Additional references
-
- Aas RW, Elliningsen KL, Lindøe P, Moller A. Leadership qualities in the return to work process: A content analysis. Journal of Occupational Rehabilitation 2008;18(4):335‐46. - PubMed
-
- Aas RW. Fast return. Evidence‐based rehabilitation of sick listed [Raskt tilbake. Kunnskapsbasert rehabilitering av sykmeldte]. [Raskt tilbake. Kunnskapsbasert rehabilitering av sykmeldte] Norwegian. Oslo: Gyldendal Akademisk, 2009.
-
- Aas RW, Thingbø C, Holte KA, Lie K, Lode IA. On long term sick leave due to musculoskeletal diseases and disorders. Experiences of work demands. Work. A journal of Prevention, Assessment and Rehabilitation 2011;(In press). - PubMed
-
- Anema JR, Steenstra IA, Bongers PM, Vet HC, Knol DL, Loisel P, Mechelen W. Multidisiplinary rehabilitation for subacute low back pain: graded activity or workplace intervention or both? A randomized controlled trial. Spine 2007;32(3):291‐98. - PubMed
-
- Ariens GA, Mechelen W, Bongers PM, Bouter LM, Wal G. Physical risk factors for neck pain. Scand J Work Environ Health 2000;26(1):7‐19. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical