

Short- and long-term outcomes after laparoscopic and open hepatic resection: systematic review and meta-analysis
- PMID: 21492329
- PMCID: PMC3093641
- DOI: 10.1111/j.1477-2574.2011.00295.x
Short- and long-term outcomes after laparoscopic and open hepatic resection: systematic review and meta-analysis
Abstract
Background: Laparoscopic liver resection (LLR) is now considered a feasible alternative to open liver resection (OLR) in selected patients. Nevertheless studies comparing LLR and OLR are few and concerns remain about long-term oncological equivalence. The present study compares outcomes with LLR vs. OLR using meta-analytical methods.
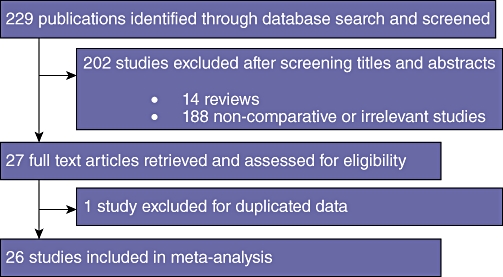
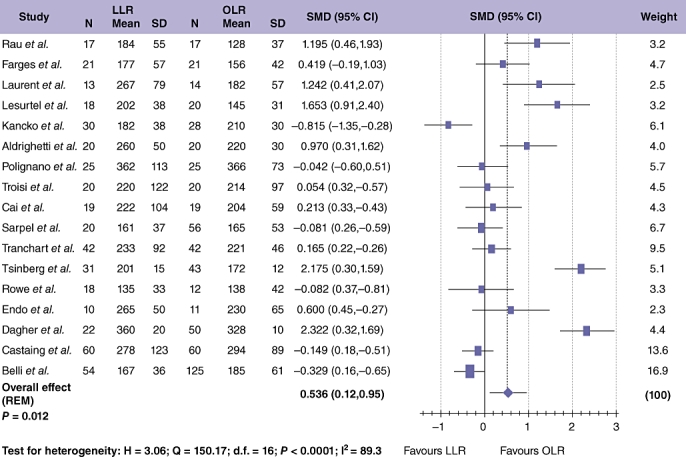
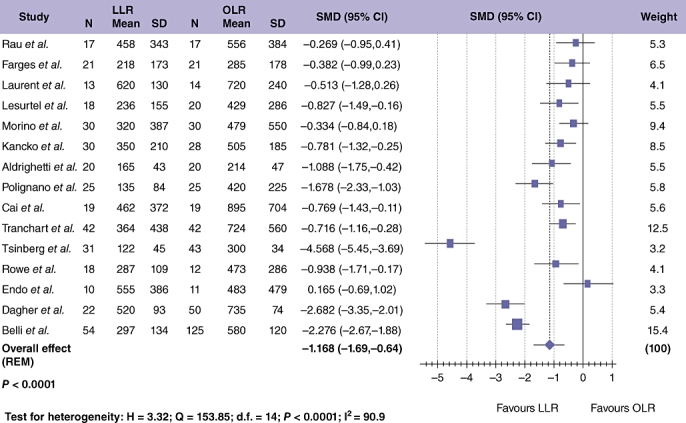
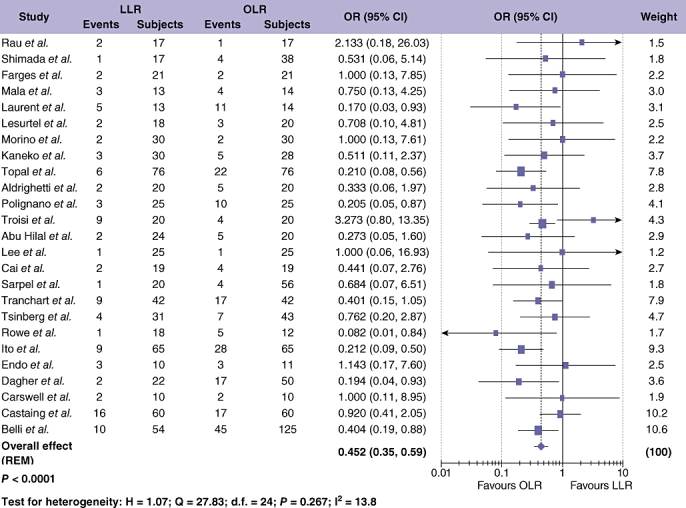
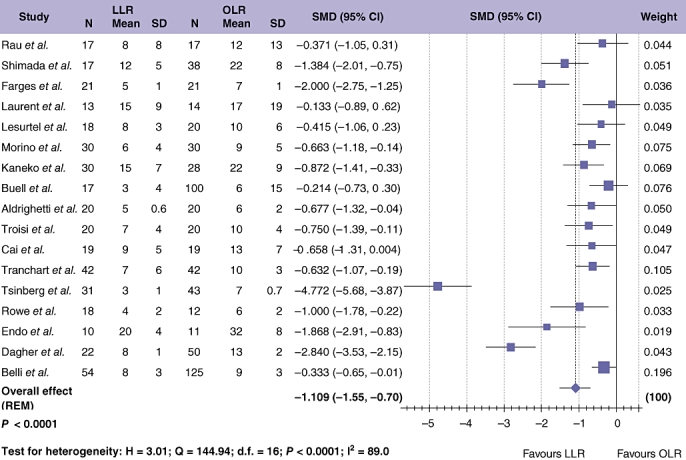
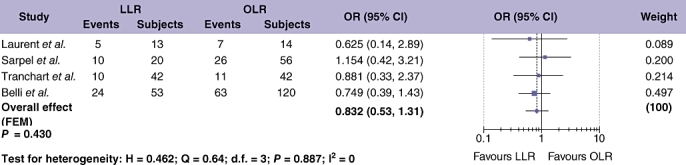
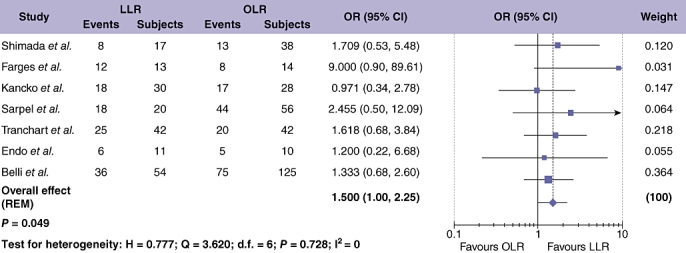
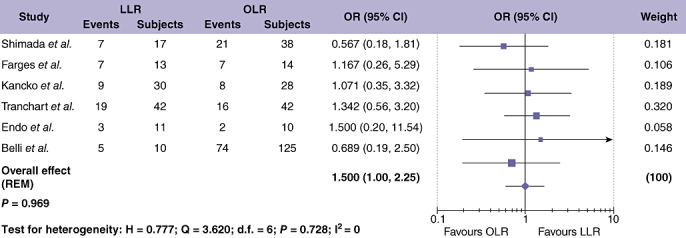
Methods: Electronic literature searches were conducted to identify studies comparing LLR and OLR. Short-term outcomes evaluated included operating time, blood loss, length of hospital stay, peri-operative morbidity and resection margin status. Longer-term outcomes included local and distant recurrence, and overall (OS) and disease-free survival (DFS). Meta-analyses were performed using the Mantel-Haenszel method and Cohen's d method, with results expressed as odds ratio (OR) or standardized mean difference (SMD), respectively, with 95% confidence intervals (CI).
Results: Twenty-six studies met the inclusion criteria with a population of 1678 patients. LLR resulted in longer operating time, but reduced blood loss, portal clamp time, overall and liver-specific complications, ileus and length of stay. No difference was found between LLR and OLR for oncological outcomes.
Discussion: LLR has short-term advantages and seemingly equivalent long-term outcomes and can be considered a feasible alternative to open surgery in experienced hands.
© 2011 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Keus F, de Jong JAF, Gooszen HG, van Laarhoven CJHM. Laparoscopic versus open cholecystectomy for patients with symptomatic cholecystolithiasis. Cochrane Database Syst Rev. 2006;(18) CD006231. - PubMed
-
- Bennett J, Boddy A, Rhodes M. Choice of approach for appendicectomy: a meta-analysis of open versus laparoscopic appendicectomy. Surg Laparosc Endosc Percutan Tech. 2007;17:245–255. - PubMed
-
- Winslow ER, Brunt LM. Perioperative outcomes of laparoscopic versus open splenectomy: a meta-analysis with an emphasis on complications. Surgery. 2003;134:647–653. discussion 654–655. - PubMed
-
- Jayne DG, Guillou PJ, Thorpe H, Quirke P, Copeland J, Smith AM, et al. UK MRC CLASICC Trial Group. Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol. 2007;25:3061–3068. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
