

LV reverse remodeling imparted by aortic valve replacement for severe aortic stenosis; is it durable? A cardiovascular MRI study sponsored by the American Heart Association
- PMID: 21492429
- PMCID: PMC3094375
- DOI: 10.1186/1749-8090-6-53
LV reverse remodeling imparted by aortic valve replacement for severe aortic stenosis; is it durable? A cardiovascular MRI study sponsored by the American Heart Association
Abstract
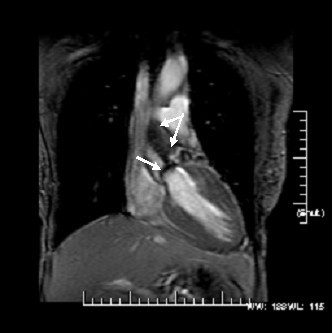
Background: In patients with severe aortic stenosis (AS), long-term data tracking surgically induced effects of afterload reduction on reverse LV remodeling are not available. Echocardiographic data is available short term, but in limited fashion beyond one year. Cardiovascular MRI (CMR) offers the ability to serially track changes in LV metrics with small numbers due to its inherent high spatial resolution and low variability.
Hypothesis: We hypothesize that changes in LV structure and function following aortic valve replacement (AVR) are detectable by CMR and once triggered by AVR, continue for an extended period.
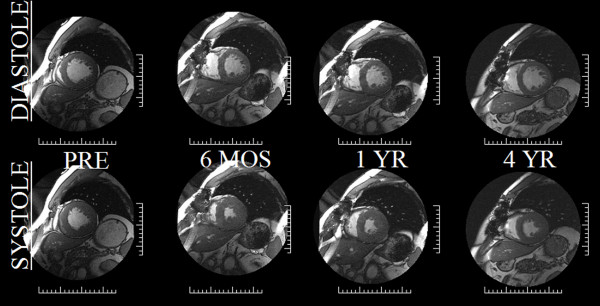
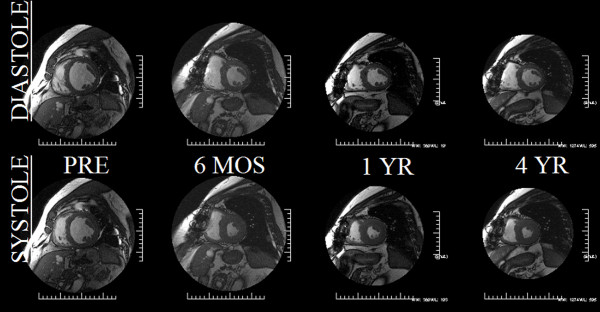
Methods: Twenty-four patients of which ten (67 ± 12 years, 6 female) with severe, but compensated AS underwent CMR pre-AVR, 6 months, 1 year and up to 4 years post-AVR. 3D LV mass index, volumetrics, LV geometry, and EF were measured.
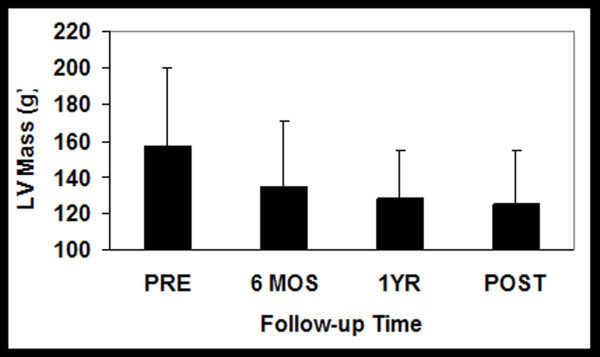
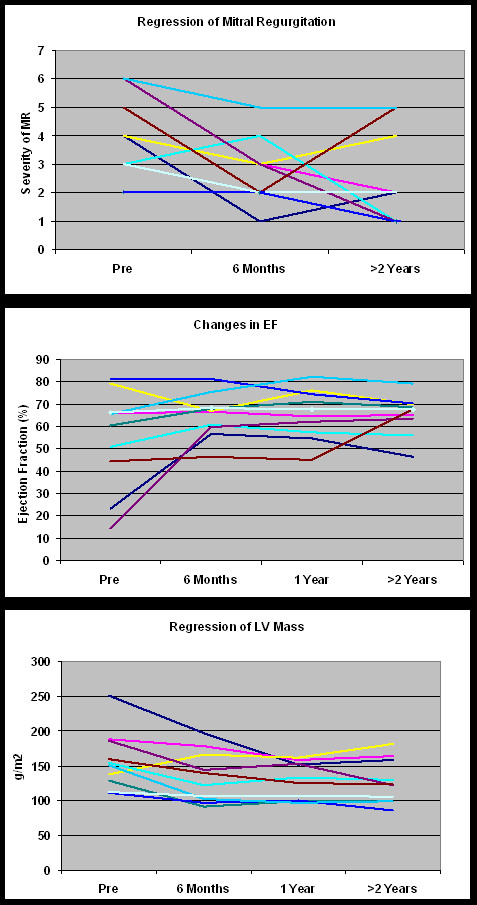
Results: All patients survived AVR and underwent CMR 4 serial CMR's. LVMI markedly decreased by 6 months (157 ± 42 to 134 ± 32 g/m2, p < 0.005) and continued trending downwards through 4 years (127 ± 32 g/m2). Similarly, EF increased pre to post-AVR (55 ± 22 to 65 ± 11%,(p < 0.05)) and continued trending upwards, remaining stable through years 1-4 (66 ± 11 vs. 65 ± 9%). LVEDVI, initially high pre-AVR, decreased post-AVR (83 ± 30 to 68 ± 11 ml/m2, p < 0.05) trending even lower by year 4 (66 ± 10 ml/m2). LV stroke volume increased rapidly from pre to post-AVR (40 ± 11 to 44 ± 7 ml, p < 0.05) continuing to increase non-significantly through 4 years (49 ± 14 ml) with these LV metrics paralleling improvements in NYHA. However, LVmass/volume, a 3D measure of LV geometry, remained unchanged over 4 years.
Conclusion: After initial beneficial effects imparted by AVR in severe AS patients, there are, as expected, marked improvements in LV reverse remodeling. Via CMR, surgically induced benefits to LV structure and function are durable and, unexpectedly express continued, albeit markedly incomplete improvement through 4 years post-AVR concordant with sustained improved clinical status. This supports down-regulation of both mRNA and MMP activity acutely with robust suppression long term.
Figures
References
-
- Lorell BH, Carabello BA. Left ventricular hypertrophy: pathogenesis, detection, and prognosis. Circ. 2000;25(4):470–9. 102. - PubMed
-
- Smucker ML, Tedesco CL, Manning SB, Owen RM, Feldman MD. Demonstration of an imbalance between coronary perfusion and excessive load as a mechanism of ischemia during stress in patients with aortic stenosis. Circ. 1988;78(3):573–82. - PubMed
-
- Nakano K, Corin WJ, Spann JF Jr, Biederman RWW, Denslow S, Carabello BA. Abnormal subendocardial blood flow in pressure overload hypertrophy is associated with pacing-induced subendocardial dysfunction. Circ Res. 1989;65(6):1555–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
