

Thick primary melanoma has a heterogeneous tumor biology: an institutional series
- PMID: 21492474
- PMCID: PMC3090362
- DOI: 10.1186/1477-7819-9-40
Thick primary melanoma has a heterogeneous tumor biology: an institutional series
Abstract
Background: Thick melanomas (TM) ≥4 mm have a high risk for nodal and distant metastases. Optimal surgical management, prognostic significance of sentinel node biopsy (SLNB), and benefits of interferon (IFN) for these patients are unclear. As a continuum of increasing tumor thickness is placed into a single TM group, differences in biologic and clinical behavior may be lost. The purpose of this study was to better characterize the diverse biology in TM, including the value of increasing thickness and nodal status information, potentially identifying high risk TM subgroups that may warrant more aggressive treatment/follow up.
Methods: 155 consecutive TM patients treated at a single institution between 1971 and 2007 were retrospectively reviewed. Patient, disease and treatment features were analyzed with respect to disease-free (DFS) and overall survival (OS).
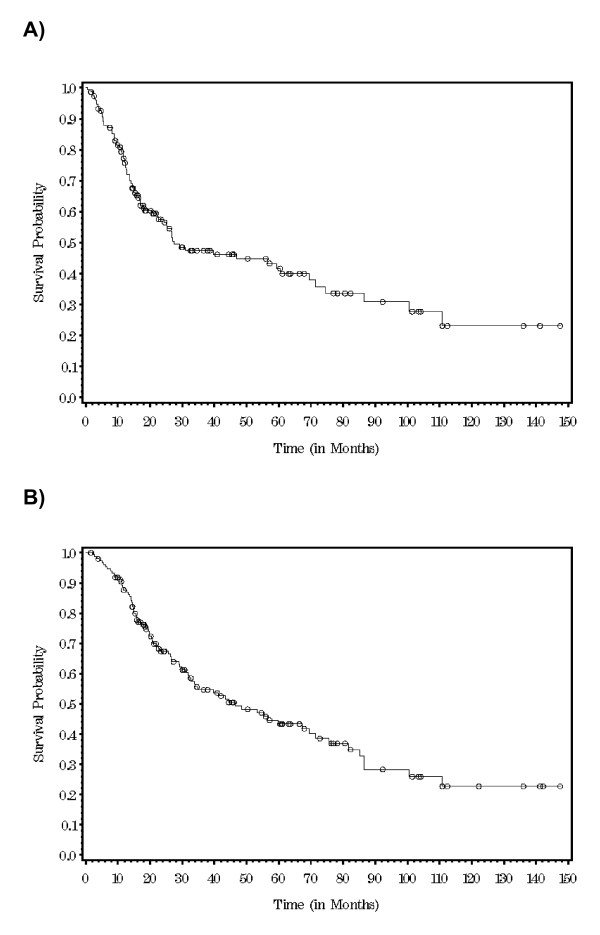
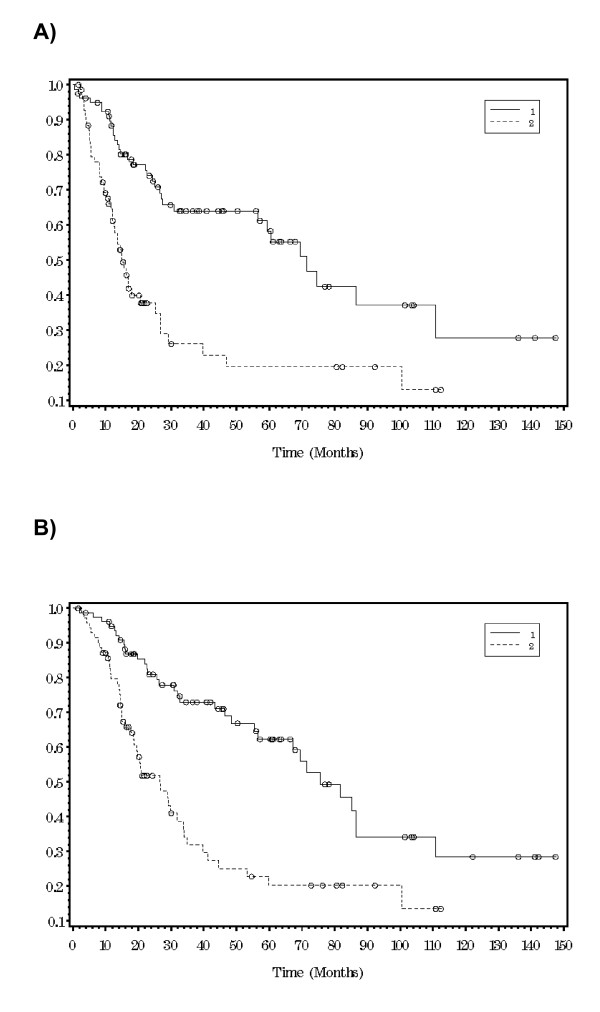
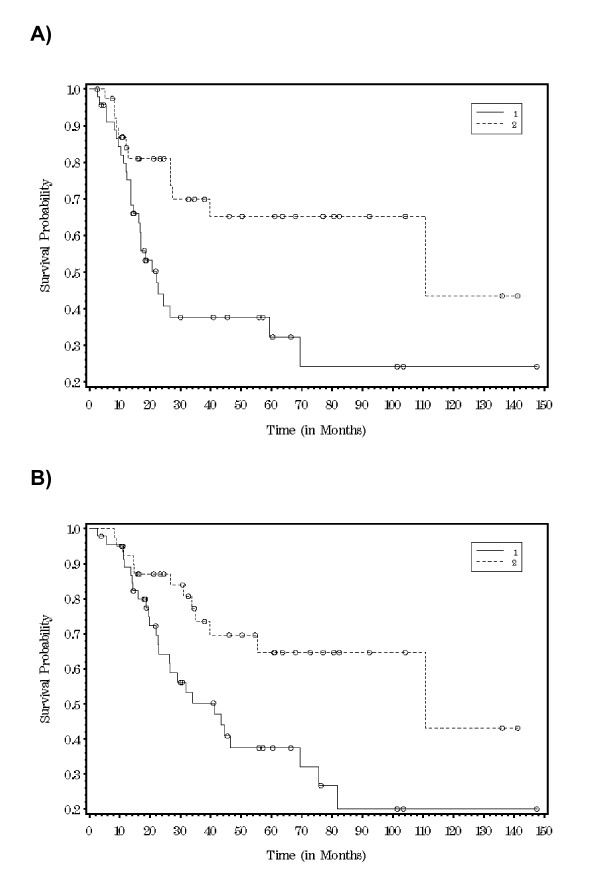
Results: Median patient age was 66 years and 68% of patients were men. The trunk was the most common TM location (35%), followed by the head and neck (29%) and lower extremities (20%). Median thickness was 6 mm and 61% were ulcerated. 6% patients had stage IV disease, 12% had clinical nodal metastases. Clinically negative lymph node basins were treated by observation (22 patients--15.4%), elective lymph node dissection (ELND) (24 patients--17.6%) or SLNB (91 patients--67%). 75% of ELND's and 53% of SLNB's were positive. Completion node dissection was performed in 38 SLNB+ patients and 22% had additional positive nodes. 17% of the study patients received IFN. At median follow up of 26 months, 5 year DFS and OS were 42% and 43.6%. For SLNB positive vs negative, median DFS were 22 vs 111 months (p = 0.006) and median OS were 41 vs 111 months (p = 0.006). When stratified by tumor thickness ≤ vs > 6 mm, 5 year DFS was 58.3% vs 20% (p < 0.0001) and OS was 62% vs 20% (P < 0.0001). IFN had no impact on DFS or OS (p = 0.98 and 0.8 respectively).
Conclusion: Within the high risk group of patients with TM, cases with tumor thickness > 6 mm or a positive SLNB had a significantly worse DFS and OS (p < .0001, <.0001 and .006, .006).
Figures
References
-
- Coit D, Sauven P, Brennan M. Prognosis of thick cutaneous melanoma of the trunk and extremity. Arch Surg. 1990;125(3):322–6. - PubMed
-
- Balch CM. et al. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. J Clin Oncol. 2001;19(16):3635–48. - PubMed
-
- Balch CM. Surgical controversies in melanoma. J Clin Oncol. 1988;6(2):392–3. - PubMed
-
- Balch CM. The role of elective lymph node dissection in melanoma: rationale, results, and controversies. J Clin Oncol. 1988;6(1):163–72. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
