

Effectiveness of a Web-based intervention aimed at healthy dietary and physical activity behavior: a randomized controlled trial about users and usage
- PMID: 21493191
- PMCID: PMC3221377
- DOI: 10.2196/jmir.1624
Effectiveness of a Web-based intervention aimed at healthy dietary and physical activity behavior: a randomized controlled trial about users and usage
Abstract
Background: Recent studies have shown the potential of Web-based interventions for changing dietary and physical activity (PA) behavior. However, the pathways of these changes are not clear. In addition, nonusage poses a threat to these interventions. Little is known of characteristics of participants that predict usage.
Objective: In this study we investigated the users and effect of the Healthy Weight Assistant (HWA), a Web-based intervention aimed at healthy dietary and PA behavior. We investigated the value of a proposed framework (including social and economic factors, condition-related factors, patient-related factors, reasons for use, and satisfaction) to predict which participants are users and which participants are nonusers. Additionally, we investigated the effectiveness of the HWA on the primary outcomes, self-reported dietary and physical activity behavior.
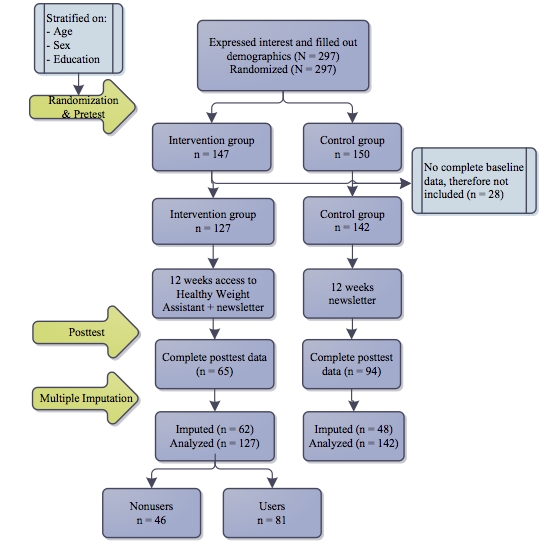
Methods: Our design was a two-armed randomized controlled trial that compared the HWA with a waiting list control condition. A total of 150 participants were allocated to the waiting list group, and 147 participants were allocated to the intervention group. Online questionnaires were filled out before the intervention period started and after the intervention period of 12 weeks. After the intervention period, respondents in the waiting list group could use the intervention. Objective usage data was obtained from the application itself.
Results: In the intervention group, 64% (81/147) of respondents used the HWA at least once and were categorized as "users." Of these, 49% (40/81) used the application only once. Increased age and not having a chronic condition increased the odds of having used the HWA (age: beta = 0.04, P = .02; chronic condition: beta = 2.24, P = .003). Within the intervention group, users scored better on dietary behavior and on knowledge about healthy behavior than nonusers (self-reported diet: χ²₂ = 8.4, P = .02; knowledge: F₁,₁₂₅ = 4.194, P = .04). Furthermore, users underestimated their behavior more often than nonusers, and nonusers overestimated their behavior more often than users (insight into dietary behavior: χ²₂ = 8.2, P = .02). Intention-to-treat analyses showed no meaningful significant effects of the intervention. Exploratory analyses of differences between pretest and posttest scores of users, nonusers, and the control group showed that on dietary behavior only the nonusers significantly improved (effect size r = -.23, P = .03), while on physical activity behavior only the users significantly improved (effect size r = -.17, P = .03).
Conclusions: Respondents did not use the application as intended. From the proposed framework, a social and economic factor (age) and a condition-related factor (chronic condition) predicted usage. Moreover, users were healthier and more knowledgeable about healthy behavior than nonusers. We found no apparent effects of the intervention, although exploratory analyses showed that choosing to use or not to use the intervention led to different outcomes. Combined with the differences between groups at baseline, this seems to imply that these groups are truly different and should be treated as separate entities.
Trial registration: Trial ID number: ISRCTN42687923; http://www.controlled-trials.com/ISRCTN42687923/ (Archived by WebCite at http://www.webcitation.org/5xnGmvQ9Y).
Conflict of interest statement
None declared
Figures
References
-
- Glenny AM, O'Meara S, Melville A, Sheldon TA, Wilson C. The treatment and prevention of obesity: a systematic review of the literature. Int J Obes Relat Metab Disord. 1997 Sep;21(9):715–37. - PubMed
-
- Hardeman W, Griffin S, Johnston M, Kinmonth AL, Wareham NJ. Interventions to prevent weight gain: a systematic review of psychological models and behaviour change methods. Int J Obes Relat Metab Disord. 2000 Feb;24(2):131–43. - PubMed
-
- Müller MJ, Asbeck I, Mast M, Langnäse K, Grund A. Prevention of obesity--more than an intention. Concept and first results of the Kiel Obesity Prevention Study (KOPS) Int J Obes Relat Metab Disord. 2001 May;25(Suppl 1):S66–74. doi: 10.1038/sj.ijo.0801703. http://dx.doi.org/10.1038/sj.ijo.0801703 - DOI - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
