

Clinically silent somatotroph adenomas are common
- PMID: 21493729
- PMCID: PMC3118490
- DOI: 10.1530/EJE-11-0216
Clinically silent somatotroph adenomas are common
Abstract
Objective: Somatotroph adenomas are typically recognized when they secrete GH excessively and cause acromegaly. Both 'silent' somatotroph adenomas (immunohistochemical evidence of GH excess without biochemical or clinical evidence) and 'clinically silent' somatotroph adenomas (immunohistochemical and biochemical evidence but no clinical evidence) have occasionally been reported. The relative frequency of each presentation is unknown. The goal of this study was, therefore, to determine the frequency of clinically silent somatotroph adenomas, a group that is potentially recognizable in vivo.
Design: We retrospectively identified 100 consecutive patients who had surgically excised and histologically confirmed pituitary adenomas.
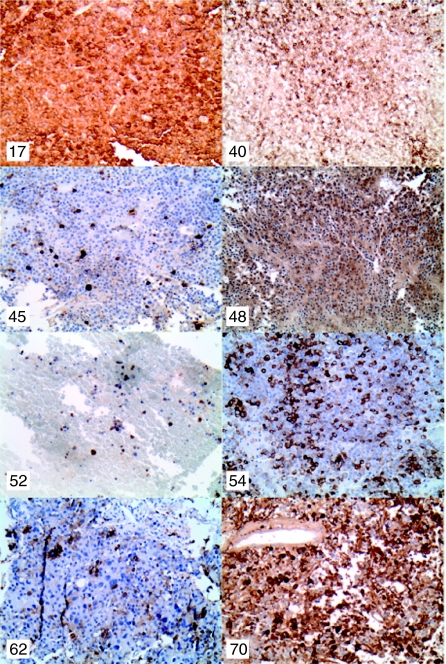
Methods: Each pituitary adenoma was classified immunohistochemically by pituitary cell type. Somatotroph adenomas were further classified as 'classic' (obvious clinical features of acromegaly and elevated serum IGF1), 'subtle' (subtle clinical features of acromegaly and elevated IGF1), 'clinically silent' (no clinical features of acromegaly but elevated IGF1), and 'silent' (no clinical features of acromegaly and normal IGF1).
Results: Of the 100 consecutive pituitary adenomas, 29% were gonadotroph/glycoprotein, 24% somatotroph, 18% null cell, 15% corticotroph, 6% lactotroph, 2% thyrotroph, and 6% not classifiable. Of the 24 patients with somatotroph adenomas, classic accounted for 45.8%, subtle 16.7%, clinically silent 33.3%, and silent 4.2%.
Conclusions: Clinically silent somatotroph adenomas are more common than previously appreciated, representing one-third of all somatotroph adenomas. IGF1 should be measured in all patients with a sellar mass, because identification of a mass as a somatotroph adenoma expands the therapeutic options and provides a tumor marker to monitor treatment.
Figures
References
-
- Kovacs K, Lloyd R, Horvath E, Asa SL, Stefaneanu L, Killinger DW, Smyth HS. Silent somatotroph adenomas of the human pituitary. A morphologic study of three cases including immunocytochemistry, electron microscopy, in vitro examination, and in situ hybridization. American Journal of Pathology. 1989;134:345–353. - PMC - PubMed
-
- Mohammed S, Syro L, Abad V, Salehi F, Horvath E, Scheithauer BW, Kovacs K, Cusimano M. Silent somatotroph adenoma of the pituitary in an adolescent. Canadian Journal of Neurological Sciences. 2009;36:123–125. - PubMed
-
- Trouillas J, Sassolas G, Loras B, Velkeniers B, Raccurt M, Chotard L, Berthezene F, Tourniaire J, Girod C. Somatotropic adenomas without acromegaly. Pathology, Research and Practice. 1991;187:943–949. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
