

Effect of nifedipine on anorectal sensorimotor functions in health and fecal incontinence
- PMID: 21493732
- PMCID: PMC3129928
- DOI: 10.1152/ajpgi.00557.2010
Effect of nifedipine on anorectal sensorimotor functions in health and fecal incontinence
Abstract
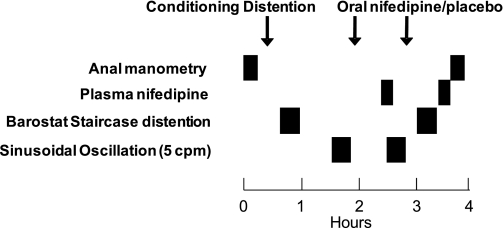
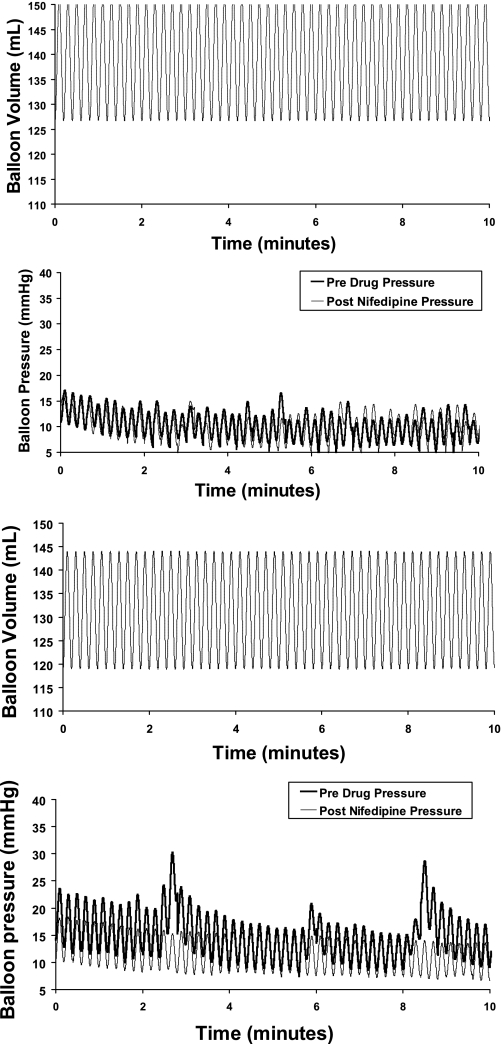
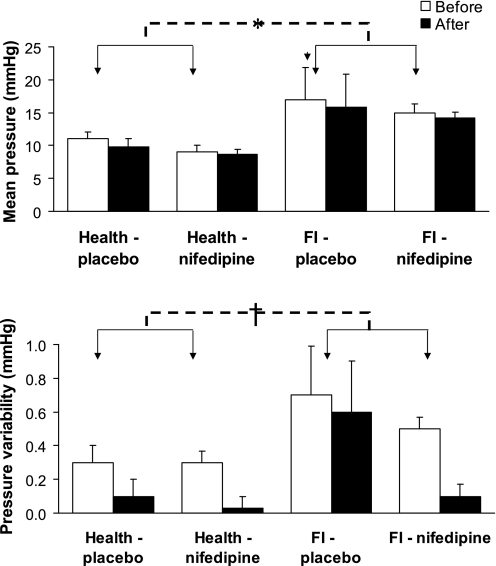
The mechanisms of increased rectal stiffness in women with fecal incontinence (FI) and rectal urgency are not understood. Our hypothesis was that distention-induced activation of mechanosensitive L-type calcium channels in smooth muscle contributes to increased rectal stiffness in FI. Anal pressures, rectal distensibility (compliance, capacity, and contractile response to sinusoidal oscillation), and rectal sensation were assessed before and after oral nifedipine (30 + 10 mg) or placebo in 16 women with FI and 16 asymptomatic women. At baseline, FI patients had a lower anal pressure increment during squeeze (health, 66.9 ± 7.6: FI, 28.6 ± 5.9, mean ± SE, P ≤ 0.01), lower rectal capacity (P = 0.052), and higher rectal pressures during sinusoidal oscillation (health, 13.7 ± 3.2: FI, 21.7 ± 1.4, mean ± SE, P = 0.02) than the healthy women, which suggests an exaggerated rectal contractile response to distention. Nifedipine decreased mean BP, increased heart rate (P = 0.01 vs. placebo), and reduced anal resting pressure (P ≤ 0.01) but did not significantly modify rectal distensibility in health or FI. Plasma nifedipine concentrations (health, 103 ± 21 ng/ml: FI, 162 ± 34 ng/ml) were correlated with increased rectal compliance (r = 0.6, P = 0.02) in all study participants and, in healthy subjects, with decreased rectal pressures during sinusoidal oscillation (r = 0.86, P = 0.01), indicative of reduced stiffness. No consistent effects on rectal perception were observed. These observations confirm that FI is associated with anal weakness and increased rectal stiffness. At therapeutic plasma concentrations, nifedipine reduced anal resting pressure but did not improve rectal distensibility in FI, outcomes that argue against a predominant contribution of myogenic L-type calcium channels to reduced rectal distensibility in FI.
Figures
Similar articles
-
A pharmacological challenge predicts reversible rectal sensorimotor dysfunctions in women with fecal incontinence.Neurogastroenterol Motil. 2018 Oct;30(10):e13383. doi: 10.1111/nmo.13383. Epub 2018 Jun 1. Neurogastroenterol Motil. 2018. PMID: 29856103 Free PMC article. Clinical Trial.
-
Rectal sensorimotor dysfunction in women with fecal incontinence.Am J Physiol Gastrointest Liver Physiol. 2007 Jan;292(1):G282-9. doi: 10.1152/ajpgi.00176.2006. Epub 2006 Aug 31. Am J Physiol Gastrointest Liver Physiol. 2007. PMID: 16950762
-
Relationship between symptoms and disordered continence mechanisms in women with idiopathic faecal incontinence.Gut. 2005 Apr;54(4):546-55. doi: 10.1136/gut.2004.047696. Gut. 2005. PMID: 15753542 Free PMC article.
-
Effects of vaginal hysterectomy on anorectal sensorimotor functions--a prospective study.Neurogastroenterol Motil. 2012 Mar;24(3):235-41. doi: 10.1111/j.1365-2982.2011.01825.x. Epub 2011 Dec 12. Neurogastroenterol Motil. 2012. PMID: 22151833 Free PMC article.
-
Pathophysiology of adult fecal incontinence.Gastroenterology. 2004 Jan;126(1 Suppl 1):S14-22. doi: 10.1053/j.gastro.2003.10.013. Gastroenterology. 2004. PMID: 14978634 Review.
Cited by
-
A novel technique for bedside anorectal manometry in humans.Neurogastroenterol Motil. 2015 Oct;27(10):1504-8. doi: 10.1111/nmo.12636. Epub 2015 Jul 30. Neurogastroenterol Motil. 2015. PMID: 26227262 Free PMC article.
-
Tools for fecal incontinence assessment: lessons for inflammatory bowel disease trials based on a systematic review.United European Gastroenterol J. 2020 Oct;8(8):886-922. doi: 10.1177/2050640620943699. Epub 2020 Jul 17. United European Gastroenterol J. 2020. PMID: 32677555 Free PMC article.
-
(2R,3S,2'' R,3''R)-manniflavanone, a new gastrointestinal smooth muscle L-type calcium channel inhibitor, which underlies the spasmolytic properties of Garcinia buchananii stem bark extract.J Smooth Muscle Res. 2014;50:48-65. doi: 10.1540/jsmr.50.48. J Smooth Muscle Res. 2014. PMID: 26081368 Free PMC article.
-
An update on anorectal disorders for gastroenterologists.Gastroenterology. 2014 Jan;146(1):37-45.e2. doi: 10.1053/j.gastro.2013.10.062. Epub 2013 Nov 6. Gastroenterology. 2014. PMID: 24211860 Free PMC article. Review.
-
A pharmacological challenge predicts reversible rectal sensorimotor dysfunctions in women with fecal incontinence.Neurogastroenterol Motil. 2018 Oct;30(10):e13383. doi: 10.1111/nmo.13383. Epub 2018 Jun 1. Neurogastroenterol Motil. 2018. PMID: 29856103 Free PMC article. Clinical Trial.
References
-
- Andrews C, Bharucha AE, Camilleri M, Low PA, Seide B, Burton D, Baxter K, Zinsmeister AR. Rectal sensorimotor dysfunction in women with fecal incontinence. Am J Physiol Gastrointest Liver Physiol 292: G282–G289, 2007 - PubMed
-
- Bassotti G, Calcara C, Annese V, Fiorella S, Roselli P, Morelli A. Nifedipine and verapamil inhibit the sigmoid colon myoelectric response to eating in healthy volunteers. Dis Colon Rectum 41: 377–380, 1998 - PubMed
-
- Bharucha AE, Dhamija S, Japp A, Seide B, Walters B, Stroetz R, Zinsmeister A, Hubmayr R. Contractile response to colonic distention is influenced by oscillation frequency. Neurogastroenterol Motil 17: 64–75, 2005 - PubMed
-
- Bharucha AE, Locke GR, Seide B, Zinsmeister AR. A new questionnaire for constipation and fecal incontinence. Alimen Pharmacol Therapeut 20: 355–364, 2004 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources