

Donor-specific antibodies accelerate arteriosclerosis after kidney transplantation
- PMID: 21493773
- PMCID: PMC3083319
- DOI: 10.1681/ASN.2010070777
Donor-specific antibodies accelerate arteriosclerosis after kidney transplantation
Abstract
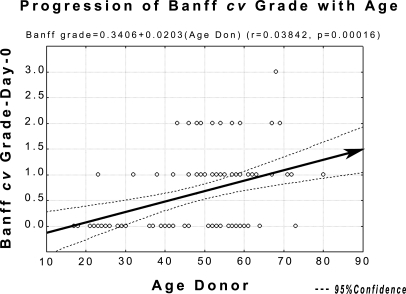
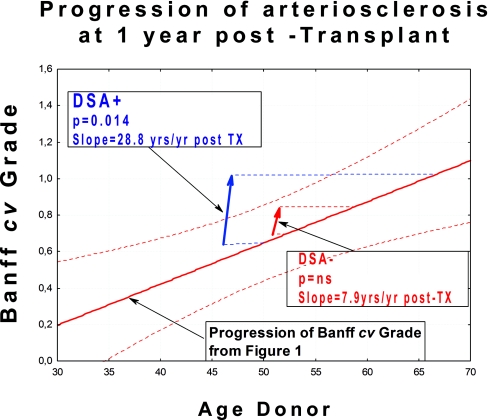
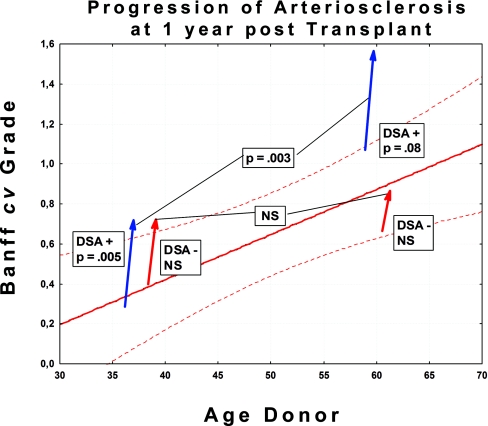
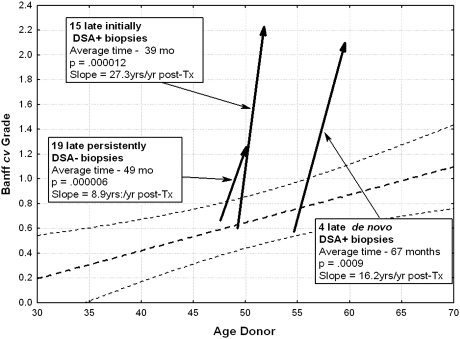
In biopsies of renal allografts, arteriosclerosis is often more severe than expected based on the age of the donor, even without a history of rejection vasculitis. To determine whether preformed donor-specific antibodies (DSAs) may contribute to the severity of arteriosclerosis, we examined protocol biopsies from patients with (n=40) or without (n=59) DSA after excluding those with any evidence of vasculitis. Among DSA-positive patients, arteriosclerosis significantly progressed between month 3 and month 12 after transplant (mean Banff cv score 0.65 ± 0.11 to 1.12 ± 0.10, P=0.014); in contrast, among DSA-negative patients, we did not detect a statistically significant progression during the same timeframe (mean Banff cv score 0.65 ± 0.11 to 0.81 ± 0.10, P=not significant). Available biopsies at later time points supported a rate of progression of arteriosclerosis in DSA-negative patients that was approximately one third that in DSA-positive patients. Accelerated arteriosclerosis was significantly associated with peritubular capillary leukocytic infiltration, glomerulitis, subclinical antibody-mediated rejection, and interstitial inflammation. In conclusion, these data support the hypothesis that donor-specific antibodies dramatically accelerate post-transplant progression of arteriosclerosis.
Copyright © 2011 by the American Society of Nephrology
Figures
References
-
- Colvin RB: Antibody-mediated renal allograft rejection: Diagnosis and pathogenesis. J Am Soc Nephrol 18: 1046–1056, 2007 - PubMed
-
- Colvin RB: Renal transplant pathology. In: Heptinstall's Pathology of the Kidney, 6th ed., edited by Jennette JC, Olson JL, Schwartz MM, Silva FG. Philadelphia, Lippincott, Williams & Wilkins, 2007, pp 1347–1490
-
- Cornell LD, Smith RN, Colvin RB: Kidney transplantation: Mechanisms of rejection and acceptance. Annu Rev Pathol 3: 189–220, 2008 - PubMed
-
- Racusen LC, Colvin RB, Solez K, Mihatsch MJ, Halloran PF, Campbell PM, Cecka MJ, Cosyns JP, Demetris AJ, Fishbein MC, Fogo A, Furness P, Gibson IW, Glotz D, Hayry P, Hunsickern L, Kashgarian M, Kerman R, Magil AJ, Montgomery R, Morozumi K, Nickeleit V, Randhawa P, Regele H, Seron D, Seshan S, Sund S, Trpkov K: Antibody-mediated rejection criteria: An addition to the Banff 97 classification of renal allograft rejection. Am J Transplant 3: 708–714, 2003 - PubMed
-
- Lefaucheur C, Nochy D, Hill GS, Glotz: Are transplant endarteritis (v1, v2) part of the spectrum of antibody-mediated rejection? [Abstract] 9th Banff Conference on Allograft Pathology, La Coruña, Spain, 2007
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
