

Regional ischemic vulnerability of the brain to hypoperfusion: the need for location specific computed tomography perfusion thresholds in acute stroke patients
- PMID: 21493917
- PMCID: PMC3090217
- DOI: 10.1161/STROKEAHA.110.600940
Regional ischemic vulnerability of the brain to hypoperfusion: the need for location specific computed tomography perfusion thresholds in acute stroke patients
Abstract
Background and purpose: To characterize the spatial pattern of cerebral ischemic vulnerability to hypoperfusion in stroke patients.
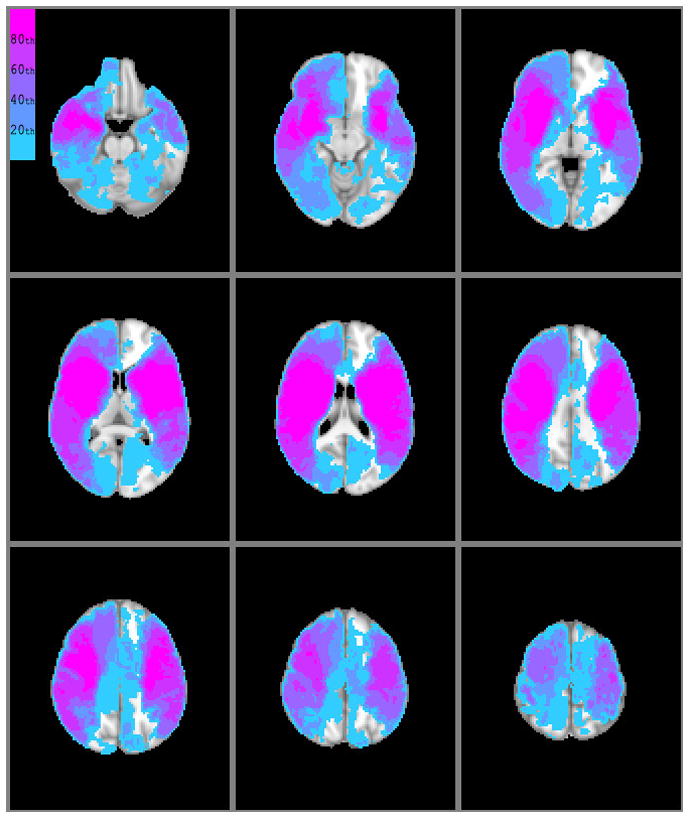
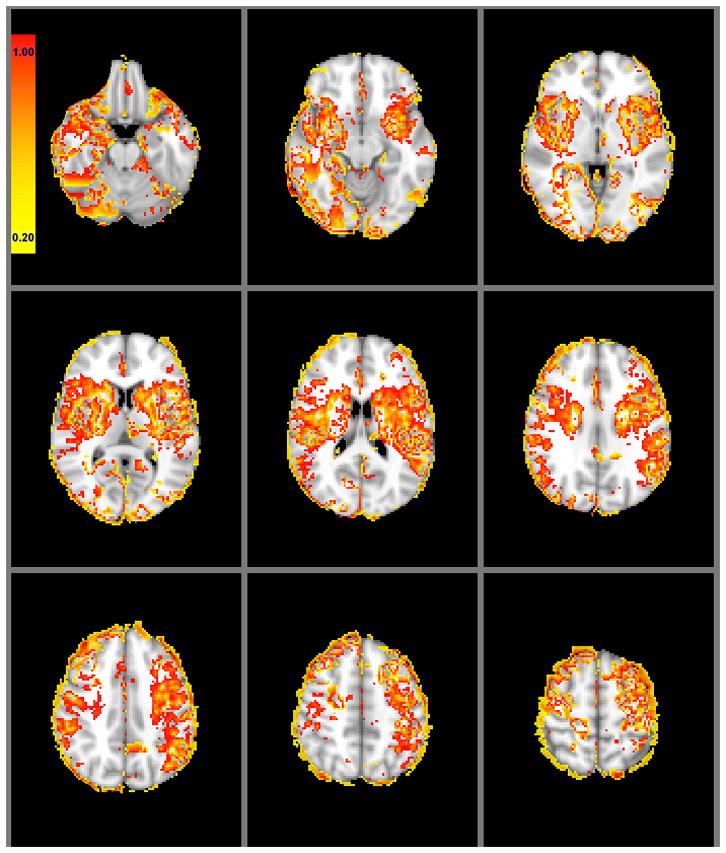
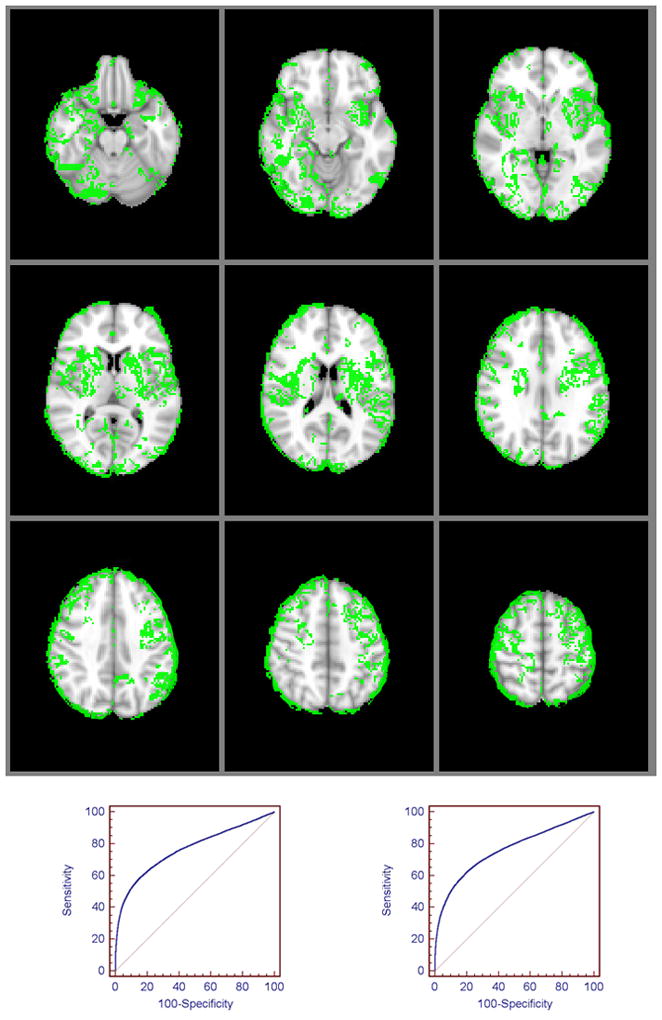
Methods: We included 90 patients who underwent admission CT perfusion and MRI within 12 hours of ischemic stroke onset. Infarcted brain lesions ("core") were segmented from admission diffusion-weighted imaging and, along with the CT perfusion parameter maps, coregistered onto MNI-152 brain space, which was parcellated into 125 mirror cortical and subcortical regions per hemisphere. We tested the hypothesis that the percent infarction increment per unit of relative cerebral blood flow (rCBF) reduction differs statistically between regions using regression analysis to assess the interaction between regional rCBF and region variables. Next, for each patient, a "vulnerability index" map was constructed with voxel values equaling the product of that voxel's rCBF and infarction probability (derived from the MNI-152-transformed, binary, segmented, diffusion-weighted imaging lesions). Voxel-based rCBF threshold for core was determined within the upper 20th percentile of vulnerability index map voxel values.
Results: Different regions had different percent infarction increase per unit rCBF reduction (P=0.001). The caudate body, putamen, insular ribbon, paracentral lobule, and precentral, middle, and inferior frontal gyri had the highest ischemic vulnerability to hypoperfusion. A voxel-based rCBF threshold of <0.42 optimally distinguished infarct core in the highly-vulnerable regions, whereas rCBF<0.16 distinguished core in the remainder of the brain.
Conclusions: We demonstrated regional ischemic vulnerability of the brain to hypoperfusion in acute stroke patients. Location-specific, rather than whole-brain, rCBF thresholds may provide a more accurate metric for estimating infarct core using CT perfusion maps.
Figures
References
-
- Marcoux FW, Morawetz RB, Crowell RM, DeGirolami U, Halsey JH., Jr Differential regional vulnerability in transient focal cerebral ischemia. Stroke. 1982;13:339–346. - PubMed
-
- Payabvash S, Kamalian S, Fung S, Wang Y, Passanese J, Souza LC, Kemmling A, Harris GJ, Halpern EF, Gonzalez RG, Furie KL, Lev MH. Predicting language improvement in acute stroke patients presenting with aphasia: A multivariate logistic model using location-weighted atlas-based analysis of admission ct perfusion scans. AJNR Am J Neuroradiol. 31:1661–1668. - PMC - PubMed
-
- Cheng B, Golsari A, Fiehler J, Rosenkranz M, Gerloff C, Thomalla G. Dynamics of regional distribution of ischemic lesions in middle cerebral artery trunk occlusion relates to collateral circulation. J Cereb Blood Flow Metab. 2010 Oct 13; doi: 10.1038/jcbfm.2010.185. [Epub ahead of print] - DOI - PMC - PubMed
-
- Dijkhuizen RM, Knollema S, van der Worp HB, Ter Horst GJ, De Wildt DJ, Berkelbach van der Sprenkel JW, Tulleken KA, Nicolay K. Dynamics of cerebral tissue injury and perfusion after temporary hypoxia-ischemia in the rat: Evidence for region-specific sensitivity and delayed damage. Stroke. 1998;29:695–704. - PubMed
