

Characterization of gap junction remodeling in epicardial border zone of healing canine infarcts and electrophysiological effects of partial reversal by rotigaptide
- PMID: 21493965
- PMCID: PMC3116056
- DOI: 10.1161/CIRCEP.110.959312
Characterization of gap junction remodeling in epicardial border zone of healing canine infarcts and electrophysiological effects of partial reversal by rotigaptide
Abstract
Background: The border zone of healing myocardial infarcts is an arrhythmogenic substrate, partly the result of structural and functional remodeling of the ventricular gap junction protein, Connexin43 (Cx43). Cx43 in arrhythmogenic substrates is a potential target for antiarrhythmic therapy.
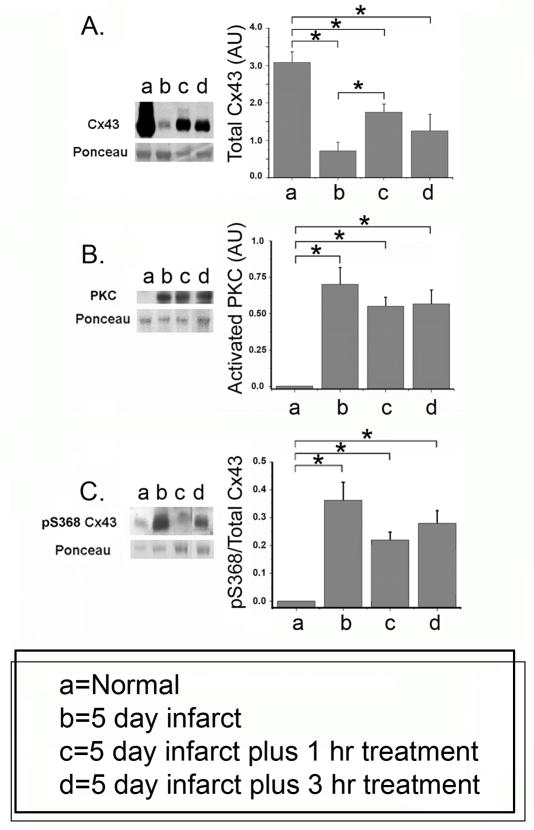
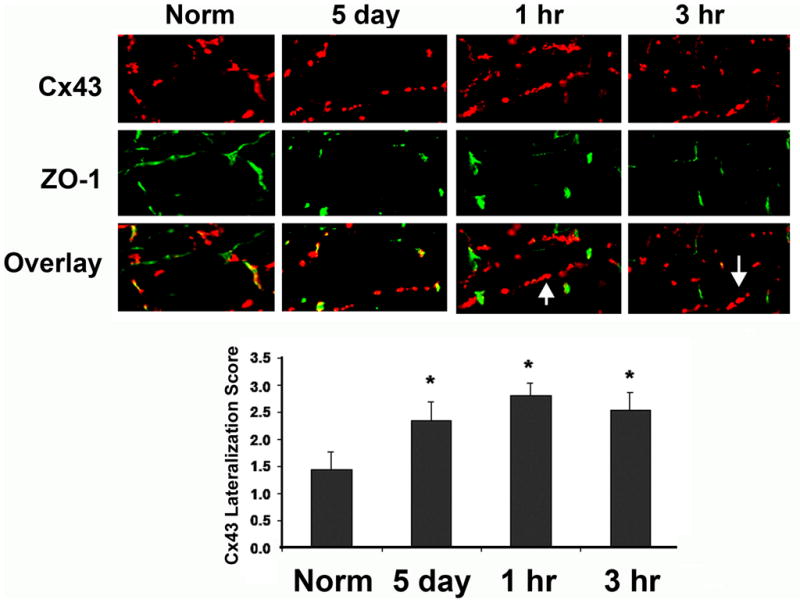
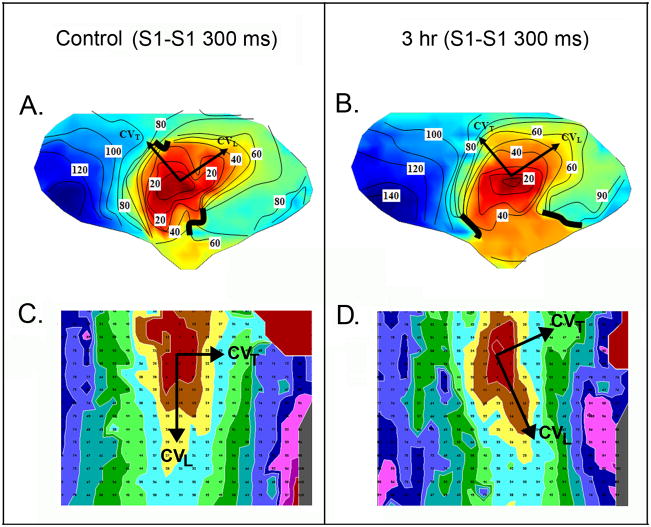
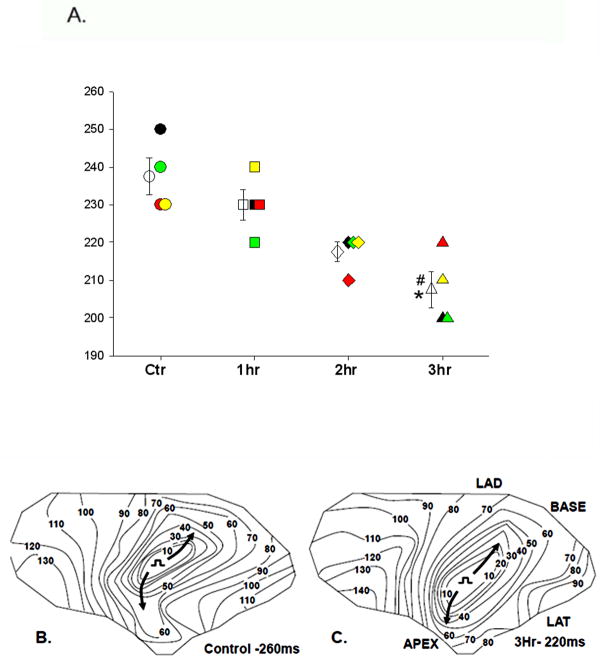
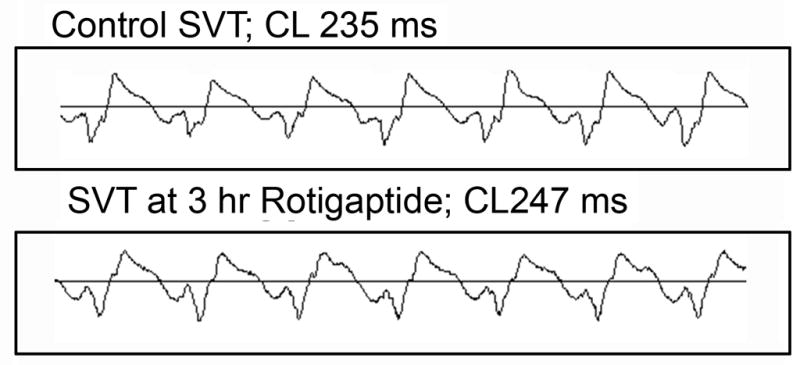
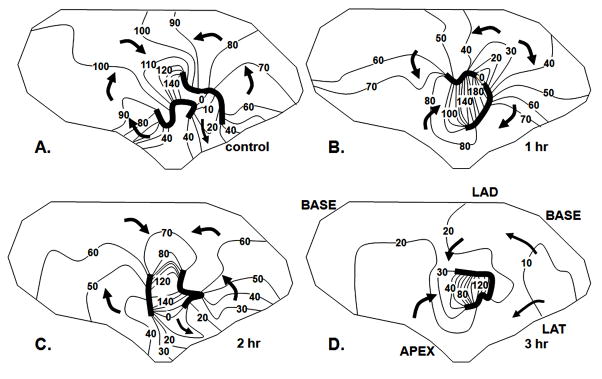
Methods and results: We characterized Cx43 remodeling in the epicardial border zone (EBZ) of healing canine infarcts 5 days after coronary occlusion and examined whether the gap junction-specific agent rotigaptide could reverse it. Cx43 remodeling in the EBZ was characterized by a decrease in Cx43 protein, lateralization, and increased Cx43 phosphorylation at serine (S) 368. Rotigaptide partially reversed the loss of Cx43 but did not affect the increase in S368 phosphorylation, nor did it reverse Cx43 lateralization. Rotigaptide did not prevent conduction slowing in the EBZ, nor did it decrease the induction of sustained ventricular tachycardia by programmed stimulation, although it did decrease the EBZ effective refractory period.
Conclusions: We conclude that partial reversal of Cx43 remodeling in healing infarct border zone may not be sufficient to restore normal conduction or prevent arrhythmias.
Conflict of interest statement
Figures
References
-
- Dillon S, Allessie M, Ursell PC, Wit AL. Influence of anisotropic tissue structure on reentrant circuits in the subepicardial border zone of subacute canine infarcts. Circulation Research. 1988;63:182–206. - PubMed
-
- Peters NS, Coromilas J, Severs NJ, Wit AL. Disturbed connexin43 gap junction distribution correlates with the location of reentrant circuits in the epicardial border zone of healing canine infarcts that cause ventricular tachycardia. Circulation. 1997;95:988–996. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
