

A universal system for highly efficient cardiac differentiation of human induced pluripotent stem cells that eliminates interline variability
- PMID: 21494607
- PMCID: PMC3072973
- DOI: 10.1371/journal.pone.0018293
A universal system for highly efficient cardiac differentiation of human induced pluripotent stem cells that eliminates interline variability
Abstract
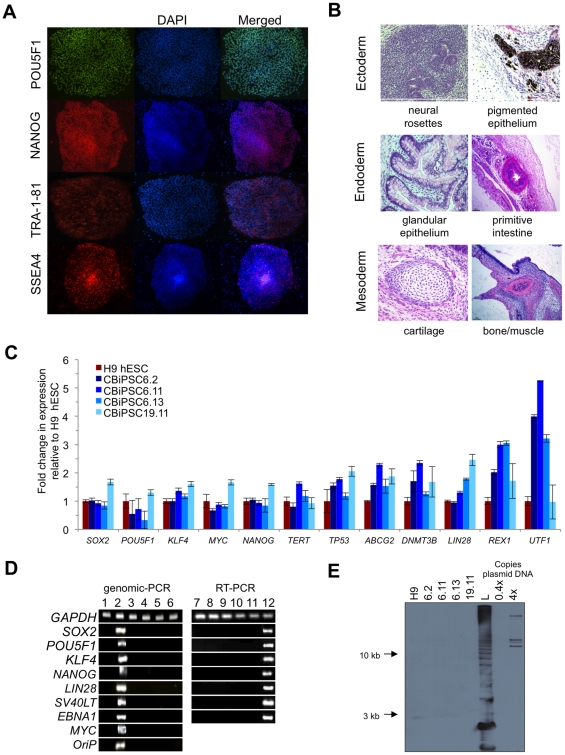
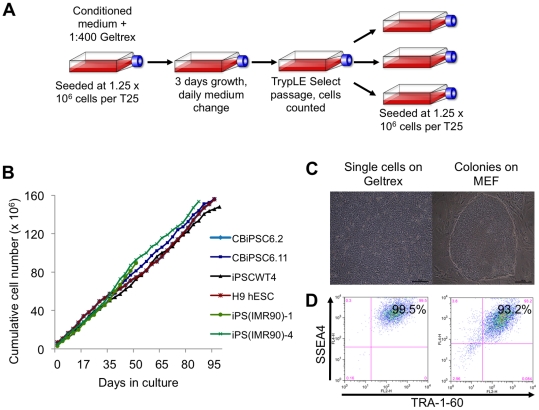
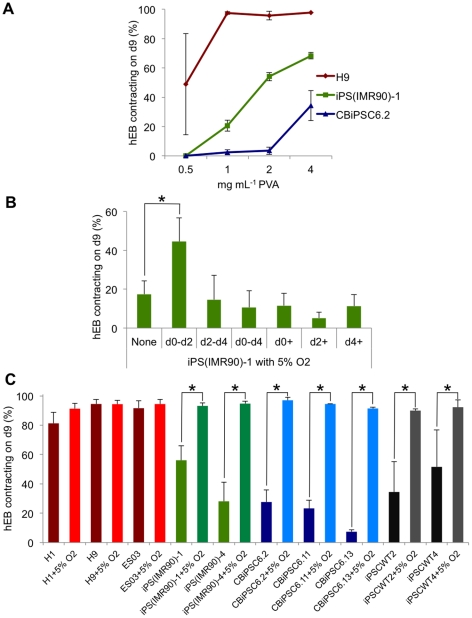
Background: The production of cardiomyocytes from human induced pluripotent stem cells (hiPSC) holds great promise for patient-specific cardiotoxicity drug testing, disease modeling, and cardiac regeneration. However, existing protocols for the differentiation of hiPSC to the cardiac lineage are inefficient and highly variable. We describe a highly efficient system for differentiation of human embryonic stem cells (hESC) and hiPSC to the cardiac lineage. This system eliminated the variability in cardiac differentiation capacity of a variety of human pluripotent stem cells (hPSC), including hiPSC generated from CD34(+) cord blood using non-viral, non-integrating methods.
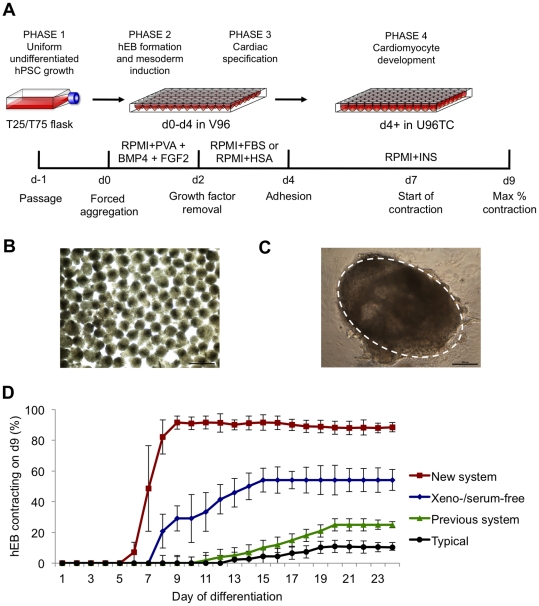
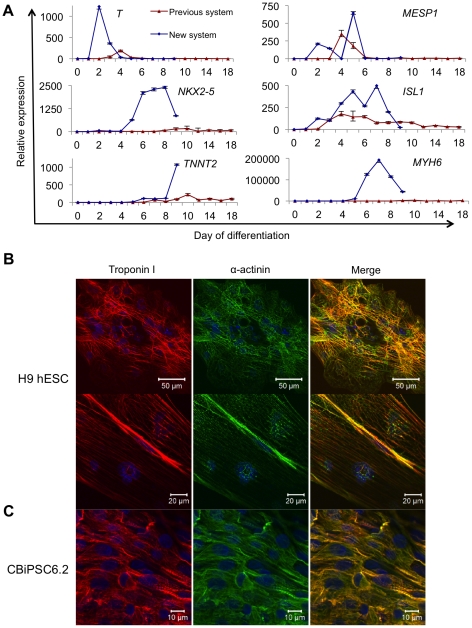
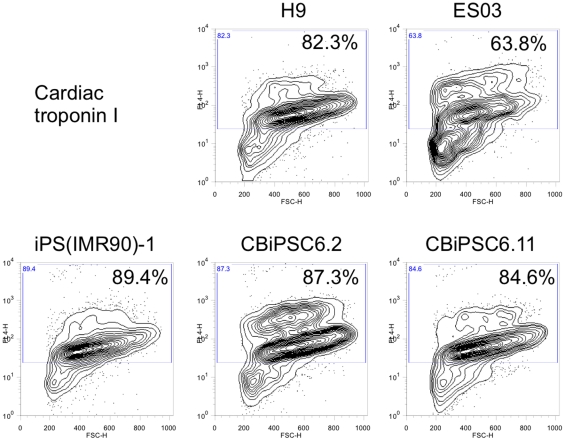
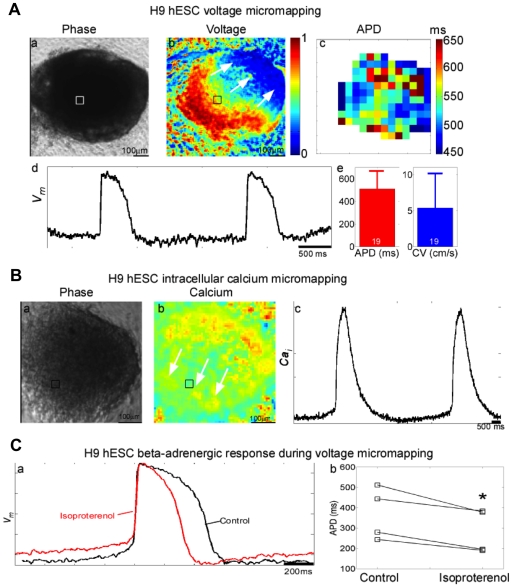
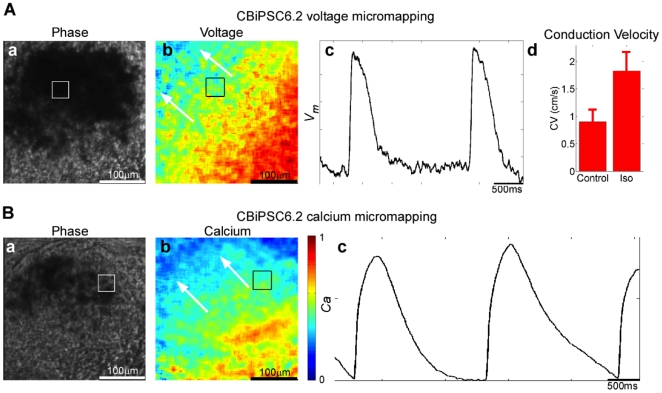
Methodology/principal findings: We systematically and rigorously optimized >45 experimental variables to develop a universal cardiac differentiation system that produced contracting human embryoid bodies (hEB) with an improved efficiency of 94.7±2.4% in an accelerated nine days from four hESC and seven hiPSC lines tested, including hiPSC derived from neonatal CD34(+) cord blood and adult fibroblasts using non-integrating episomal plasmids. This cost-effective differentiation method employed forced aggregation hEB formation in a chemically defined medium, along with staged exposure to physiological (5%) oxygen, and optimized concentrations of mesodermal morphogens BMP4 and FGF2, polyvinyl alcohol, serum, and insulin. The contracting hEB derived using these methods were composed of high percentages (64-89%) of cardiac troponin I(+) cells that displayed ultrastructural properties of functional cardiomyocytes and uniform electrophysiological profiles responsive to cardioactive drugs.
Conclusion/significance: This efficient and cost-effective universal system for cardiac differentiation of hiPSC allows a potentially unlimited production of functional cardiomyocytes suitable for application to hPSC-based drug development, cardiac disease modeling, and the future generation of clinically-safe nonviral human cardiac cells for regenerative medicine.
Conflict of interest statement
Figures
Comment in
-
Induced pluripotent stem cells: progress towards a biomedical application.Expert Rev Cardiovasc Ther. 2011 Oct;9(10):1265-9. doi: 10.1586/erc.11.123. Expert Rev Cardiovasc Ther. 2011. PMID: 21985539
References
-
- Hansson EM, Lindsay ME, Chien KR. Regeneration next: toward heart stem cell therapeutics. Cell Stem Cell. 2009;5:364–377. - PubMed
-
- Kehat I, Gepstein A, Spira A, Itskovitz-Eldor J, Gepstein L. High-resolution electrophysiological assessment of human embryonic stem cell-derived cardiomyocytes: a novel in vitro model for the study of conduction. Circ Res. 2002;91:659–661. - PubMed
-
- Xu C, Police S, Rao N, Carpenter MK. Characterization and enrichment of cardiomyocytes derived from human embryonic stem cells. Circ Res. 2002;91:501–508. - PubMed
-
- Mummery C, Ward-van Oostwaard D, Doevendans P, Spijker R, van den Brink S, et al. Differentiation of human embryonic stem cells to cardiomyocytes: role of coculture with visceral endoderm-like cells. Circulation. 2003;107:2733–2740. - PubMed
-
- Braam SR, Tertoolen L, van de Stolpe A, Meyer T, Passier R, et al. Prediction of drug-induced cardiotoxicity using human embryonic stem cell-derived cardiomyocytes. Stem Cell Res. 2010;4:107–116. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
