

Targeted morphoproteomic profiling of Ewing's sarcoma treated with insulin-like growth factor 1 receptor (IGF1R) inhibitors: response/resistance signatures
- PMID: 21494688
- PMCID: PMC3071831
- DOI: 10.1371/journal.pone.0018424
Targeted morphoproteomic profiling of Ewing's sarcoma treated with insulin-like growth factor 1 receptor (IGF1R) inhibitors: response/resistance signatures
Abstract
Background: Insulin-like growth factor 1 receptor (IGF1R) targeted therapies have resulted in responses in a small number of patients with advanced metastatic Ewing's sarcoma. We performed morphoproteomic profiling to better understand response/resistance mechanisms of Ewing's sarcoma to IGF1R inhibitor-based therapy.
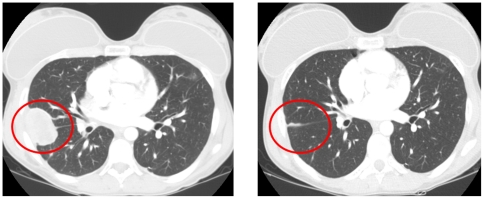
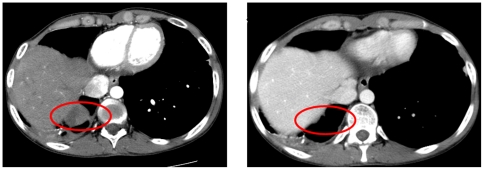
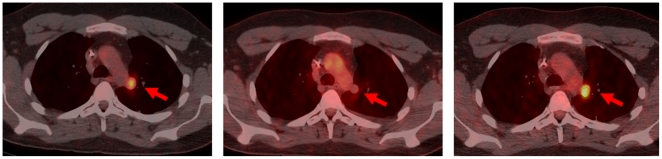
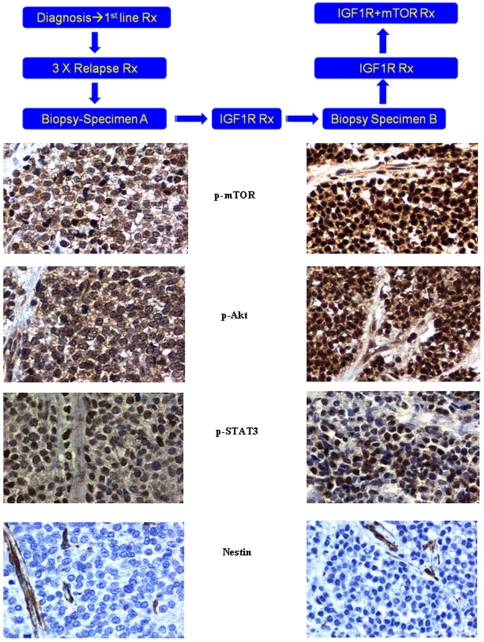
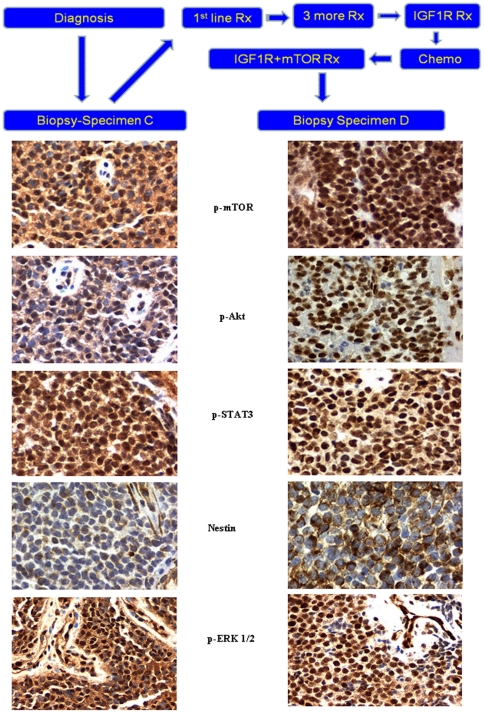
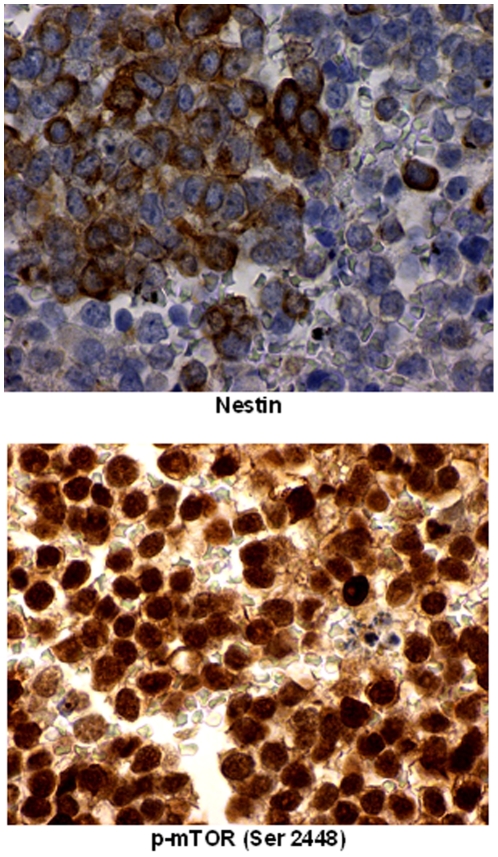
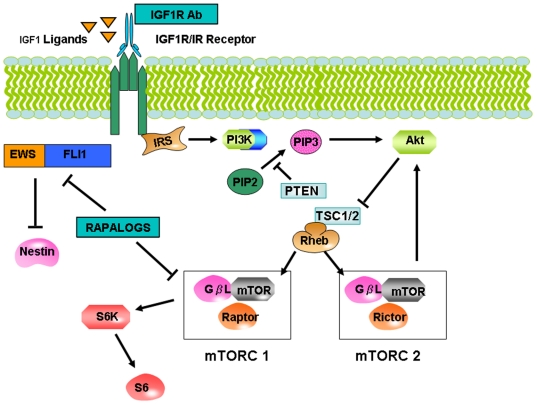
Methodology/principal findings: This pilot study assessed two patients with advanced Ewing's sarcoma treated with IGF1R antibody alone followed by combined IGF1R inhibitor plus mammalian target of rapamycin (mTOR) inhibitor treatment once resistance to single-agent IGF1R inhibitor developed. Immunohistochemical probes were applied to detect p-mTOR (Ser2448), p-Akt (Ser473), p-ERK1/2 (Thr202/Tyr204), nestin, and p-STAT3 (Tyr 705) in the original and recurrent tumor. The initial remarkable radiographic responses to IGF1R-antibody therapy was followed by resistance and then response to combined IGF1R plus mTOR inhibitor therapy in both patients, and then resistance to the combination regimen in one patient. In patient 1, upregulation of p-Akt and p-mTOR in the tumor that relapsed after initial response to IGF1R antibody might explain the resistance that developed, and the subsequent response to combined IGF1R plus mTOR inhibitor therapy. In patient 2, upregulation of mTOR was seen in the primary tumor, perhaps explaining the initial response to the IGF1R and mTOR inhibitor combination, while the resistant tumor that emerged showed activation of the ERK pathway as well.
Conclusion/significance: Morphoproteomic analysis revealed that the mTOR pathway was activated in these two patients with advanced Ewing's sarcoma who showed response to combined IGF1R and mTOR inhibition, and the ERK pathway in the patient in whom resistance to this combination emerged. Our pilot results suggests that morphoproteomic assessment of signaling pathway activation in Ewing's sarcoma merits further investigation as a guide to understanding response and resistance signatures.
Conflict of interest statement
Figures
References
-
- Balamuth NJ, Womer RB. Ewing's sarcoma. Lancet Oncol. 2010;11:184–192. - PubMed
-
- Subbiah V, Anderson P, Lazar AJ, Burdett E, Raymond K, et al. Ewing's sarcoma: standard and experimental treatment options. Curr Treat Options Oncol. 2009;10:126–140. - PubMed
-
- Ludwig JA. Ewing sarcoma: historical perspectives, current state-of-the-art, and opportunities for targeted therapy in the future. Curr Opin Oncol. 2008;20:412–418. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
