

Skeletal findings in children recently initiating glucocorticoids for the treatment of nephrotic syndrome
- PMID: 21494860
- PMCID: PMC4000256
- DOI: 10.1007/s00198-011-1621-2
Skeletal findings in children recently initiating glucocorticoids for the treatment of nephrotic syndrome
Abstract
Summary: Eighty children with nephrotic syndrome underwent lumbar spine densitometry and vertebral morphometry soon after glucocorticoid initiation. We found an inverse relationship between glucocorticoid exposure and spine areal bone mineral density (BMD) Z-score and a low rate of vertebral deformities (8%).
Introduction: Vertebral fractures are an under-recognized complication of childhood glucocorticoid-treated illnesses. Our goal was to study the relationships among glucocorticoid exposure, lumbar spine areal BMD (LS BMD), and vertebral shape in glucocorticoid-treated children with new-onset nephrotic syndrome.
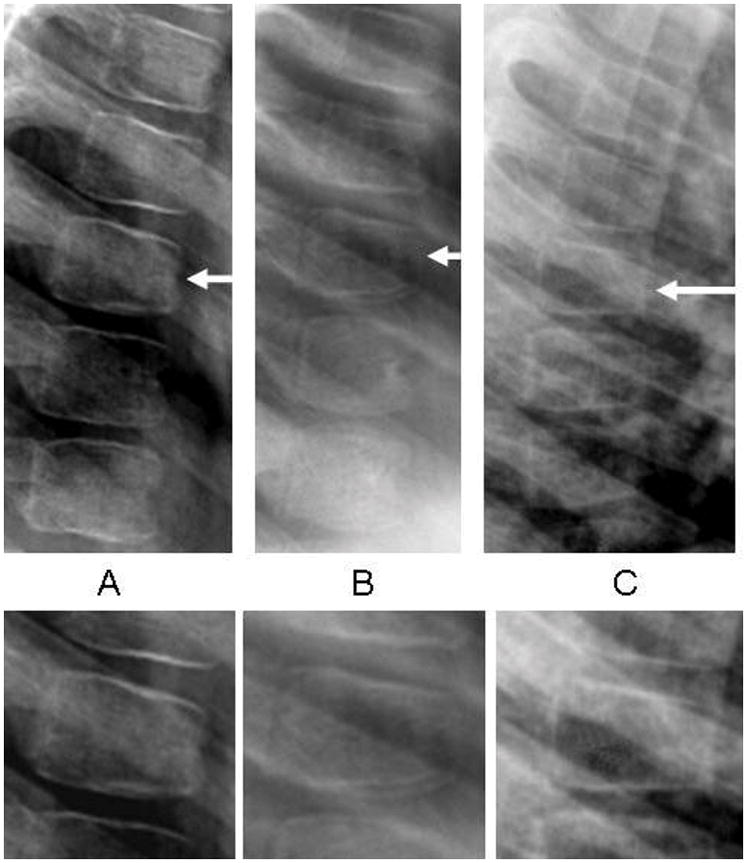
Methods: Lateral thoracolumbar spine radiography and LS BMD were performed in 80 children with nephrotic syndrome (median age 4.4 years; 46 boys) within the first 37 days of glucocorticoid therapy. Genant semiquantitative grading was used as the primary method for vertebral morphometry; the algorithm-based qualitative (ABQ) method was used for secondary vertebral deformity analysis.
Results: Six of the 78 children with usable radiographs (8%; 95% confidence interval 4 to 16%) manifested a single Genant grade 1 deformity each. All deformities were mild anterior wedging (two at each of T6, T7, and T8). Four of the 78 children (5%; 95% confidence interval 2 to 13%) showed one ABQ sign of fracture each (loss of endplate parallelism; two children at T6 and two at T8). Two of the children with ABQ signs also had a Genant grade 1 deformity in the same vertebral body. None of the children with a Genant or ABQ deformity reported back pain. An inverse relationship was identified between LS BMD Z-score and glucocorticoid exposure.
Conclusions: Although we identified an inverse relationship between steroid exposure and LS BMD soon after glucocorticoid initiation for childhood nephrotic syndrome, there was only a low rate of vertebral deformities. The clinical significance of these findings requires further study.
Conflict of interest statement
None of the authors has a conflict of interest
Figures
References
-
- Schlesinger ER, Sultz HA, Mosher WE, Feldman JG. The nephrotic syndrome. Its incidence and implications for the community. Am J Dis Child. 1968;116:623–632. - PubMed
-
- Hodson EM, Knight JF, Willis NS, Craig JC. Corticosteroid therapy for nephrotic syndrome in children. Cochrane Database Syst Rev. 2001;2 - PubMed
-
- Clark AG, Barratt TM. Steroid-responsive nephrotic syndrome. In: Barratt TM, Avner ED, Harmon WE, editors. Pediatric Nephrology. 4. 1999. pp. 731–747.
-
- van Staa TP, Cooper C, Leufkens HG, Bishop N. Children and the risk of fractures caused by oral corticosteroids. J Bone Miner Res. 2003;18:913–918. - PubMed
-
- Dalle Carbonare L, Arlot ME, Chavassieux PM, Roux JP, Portero NR, Meunier PJ. Comparison of trabecular bone microarchitecture and remodeling in glucocorticoid-induced and postmenopausal osteoporosis. J Bone Miner Res. 2001;16:97–103. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
