

Predicting 30-day mortality of aortic valve replacement by the AVR score
- PMID: 21494889
- PMCID: PMC3111570
- DOI: 10.1007/s12471-011-0103-7
Predicting 30-day mortality of aortic valve replacement by the AVR score
Abstract
Objectives: The objective of this study is to develop a simple risk score to predict 30-day mortality of aortic valve replacement (AVR).
Methods: In a development set of 673 consecutive patients who underwent AVR between 1990 and 1993, four independent predictors for 30-day mortality were identified: body mass index (BMI) ≥30, BMI <20, previous coronary artery bypass grafting (CABG) and recent myocardial infarction. Based on these predictors, a 30-day mortality risk score-the AVR score-was developed. The AVR score was validated on a validation set of 673 consecutive patients who underwent AVR almost two decennia later in the same hospital.
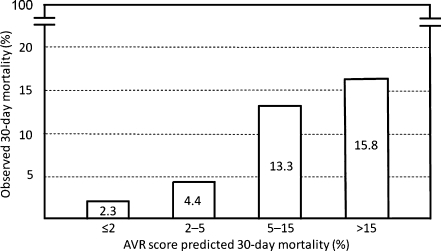
Results: Thirty-day mortality in the development set was ≤2% in the absence of any predictor (class I, low risk), 2-5% in the solitary presence of BMI ≥30 (class II, mild risk), 5-15% in the solitary presence of previous CABG or recent myocardial infarction (class III, moderate risk), and >15% in the solitary presence of BMI <20, or any combination of BMI ≥30, previous CABG or recent myocardial infarction (class IV, high risk). The AVR score correctly predicted 30-day mortality in the validation set: observed 30-day mortality in the validation set was 2.3% in 487 class I patients, 4.4% in 137 class II patients, 13.3% in 30 class III patients and 15.8% in 19 class IV patients.
Conclusions: The AVR score is a simple risk score validated to predict 30-day mortality of AVR.
Figures
Similar articles
-
Aortic valve replacement after previous coronary artery bypass grafting.Ann Thorac Surg. 1996 Nov;62(5):1424-30. doi: 10.1016/0003-4975(96)00635-2. Ann Thorac Surg. 1996. PMID: 8893579 Review.
-
Does additional coronary artery bypass grafting to aortic valve replacement in elderly patients affect the early and long-term outcome?Heart Vessels. 2020 Apr;35(4):487-501. doi: 10.1007/s00380-019-01519-6. Epub 2019 Oct 18. Heart Vessels. 2020. PMID: 31642980 Free PMC article.
-
Early results of aortic valve replacement with or without concomitant coronary artery bypass grafting.Scand J Thorac Cardiovasc Surg. 1991;25(1):29-35. doi: 10.3109/14017439109098080. Scand J Thorac Cardiovasc Surg. 1991. PMID: 2063151
-
Moderate aortic stenosis in coronary artery bypass grafting patients more than 70 years of age: to replace or not to replace?Ann Thorac Surg. 2010 Nov;90(5):1495-9; discussion 1499-500. doi: 10.1016/j.athoracsur.2010.06.036. Ann Thorac Surg. 2010. PMID: 20971247
-
Management of Less-Than-Severe Aortic Stenosis During Coronary Bypass: A Systematic Review and Meta-Analysis.Innovations (Phila). 2019 Aug;14(4):291-298. doi: 10.1177/1556984519849639. Epub 2019 Jun 11. Innovations (Phila). 2019. PMID: 31185776
Cited by
-
The impact of nutritional status and appetite on the hospital length of stay and postoperative complications in elderly patients with severe aortic stenosis before aortic valve replacement.Kardiochir Torakochirurgia Pol. 2016 Jun;13(2):105-12. doi: 10.5114/kitp.2016.61042. Epub 2016 Jun 30. Kardiochir Torakochirurgia Pol. 2016. PMID: 27516781 Free PMC article.
-
What Can We Learn from the Past by Means of Very Long-Term Follow-Up after Aortic Valve Replacement?J Clin Med. 2021 Aug 31;10(17):3925. doi: 10.3390/jcm10173925. J Clin Med. 2021. PMID: 34501375 Free PMC article.
References
-
- Shahian DM, O’Brien SM, Filardo G, Society of Thoracic Surgeons Quality Measurement Task Force et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 1–coronary artery bypass grafting surgery. Ann Thorac Surg. 2009;88:S2–S22. doi: 10.1016/j.athoracsur.2009.05.053. - DOI - PubMed
LinkOut - more resources
Full Text Sources
