

End-of-life care in Medicare beneficiaries dying with pancreatic cancer
- PMID: 21495020
- PMCID: PMC3139734
- DOI: 10.1002/cncr.26115
End-of-life care in Medicare beneficiaries dying with pancreatic cancer
Abstract
Background: The authors' goal was to characterize hospice enrollment and aggressiveness of care for pancreatic cancer patients at the end of life.
Methods: Surveillance, Epidemiology, and End Results and linked Medicare claims data (1992-2006) were used to identify patients with pancreatic cancer who had died (n = 22,818). The authors evaluated hospice use, hospice enrollment ≥ 4 weeks before death, and aggressiveness of care as measured by receipt of chemotherapy, acute care hospitalization, and intensive care unit (ICU) admission in the last month of life.
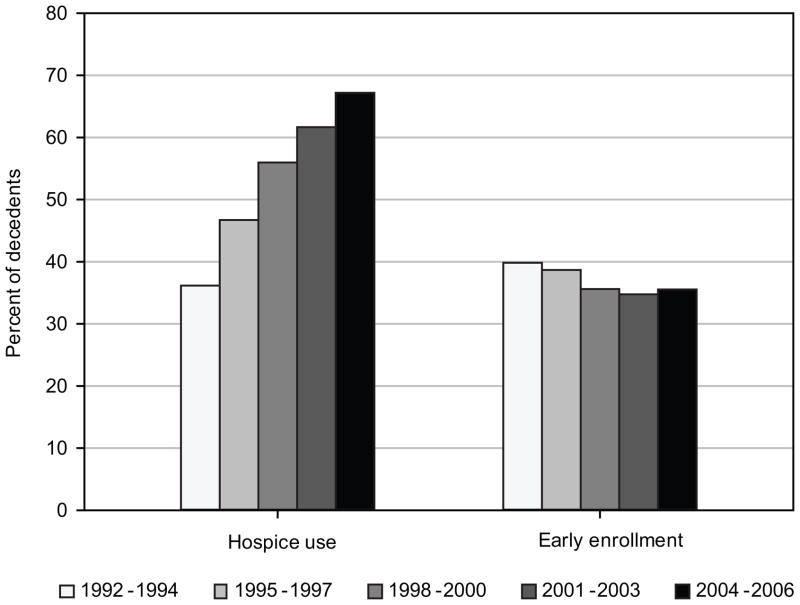
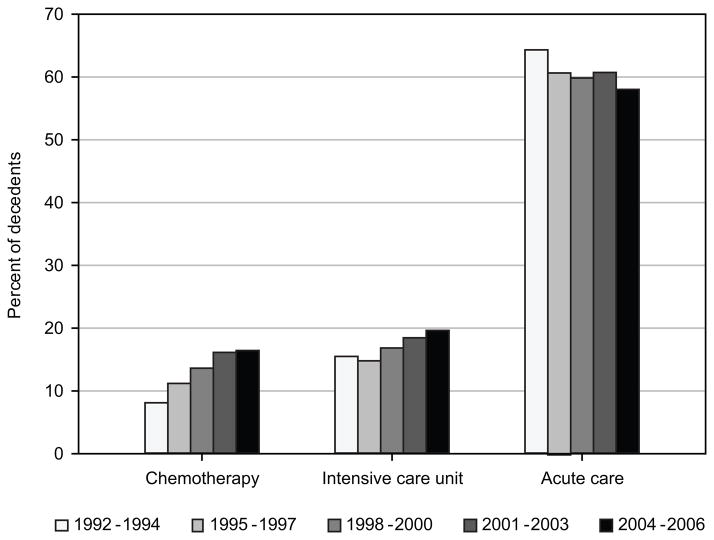
Results: Overall, 56.9% of patients enrolled in hospice, and 35.9% of hospice users enrolled for 4 weeks or more. Hospice use increased from 36.2% in 1992-1994 to 67.2% in 2004-2006 (P < .0001). Admission to the ICU and receipt of chemotherapy in the last month of life increased from 15.5% to 19.6% (P < .0001) and from 8.1% to 16.4% (P < .0001), respectively. Among patients with locoregional disease, those who underwent resection were less likely to enroll in hospice before death and much less likely to enroll early. They were also more likely to receive chemotherapy (14% vs 9%, P < .0001), be admitted to an acute care hospital (61% vs 53%, P < .0001), and be admitted to an ICU (27% vs 15%, P < .0001) in the last month of life.
Conclusions: Although hospice use increased over time, there was a simultaneous decrease in early enrollment and increase in aggressive care at the end of life for patients with pancreatic cancer.
Copyright © 2011 American Cancer Society.
Figures
Similar articles
-
Association Between Hospice Length of Stay, Health Care Utilization, and Medicare Costs at the End of Life Among Patients Who Received Maintenance Hemodialysis.JAMA Intern Med. 2018 Jun 1;178(6):792-799. doi: 10.1001/jamainternmed.2018.0256. JAMA Intern Med. 2018. PMID: 29710217 Free PMC article.
-
Family Perspectives on Aggressive Cancer Care Near the End of Life.JAMA. 2016 Jan 19;315(3):284-92. doi: 10.1001/jama.2015.18604. JAMA. 2016. PMID: 26784776 Free PMC article.
-
Hospice utilization among Medicare beneficiaries dying from pancreatic cancer.J Surg Oncol. 2019 Sep;120(4):624-631. doi: 10.1002/jso.25623. Epub 2019 Jul 9. J Surg Oncol. 2019. PMID: 31290170
-
Patterns and predictors of end-of-life care in older patients with pancreatic cancer.Cancer Med. 2018 Dec;7(12):6401-6410. doi: 10.1002/cam4.1861. Epub 2018 Nov 13. Cancer Med. 2018. PMID: 30426697 Free PMC article.
-
Continuity of care and receipt of aggressive end of life care among women dying of ovarian cancer.Gynecol Oncol. 2021 Jul;162(1):148-153. doi: 10.1016/j.ygyno.2021.04.024. Epub 2021 Apr 28. Gynecol Oncol. 2021. PMID: 33931242 Free PMC article.
Cited by
-
Hospital and medical care days in pancreatic cancer.Ann Surg Oncol. 2012 Aug;19(8):2435-42. doi: 10.1245/s10434-012-2326-2. Epub 2012 Mar 27. Ann Surg Oncol. 2012. PMID: 22451235 Free PMC article.
-
Measuring intensity of end of life care: a systematic review.PLoS One. 2015 Apr 14;10(4):e0123764. doi: 10.1371/journal.pone.0123764. eCollection 2015. PLoS One. 2015. PMID: 25875471 Free PMC article.
-
Initial treatment is associated with improved survival and end-of-life outcomes for patients with pancreatic cancer: a cohort study.BMC Cancer. 2022 Dec 14;22(1):1312. doi: 10.1186/s12885-022-10342-8. BMC Cancer. 2022. PMID: 36517794 Free PMC article.
-
Frequency of anticancer drug use at the end of life: a scoping review.Clin Transl Oncol. 2024 Jan;26(1):178-189. doi: 10.1007/s12094-023-03234-1. Epub 2023 Jun 8. Clin Transl Oncol. 2024. PMID: 37286888 Free PMC article.
-
End-of-Life Cancer Care Resource Utilisation in Rural Versus Urban Settings: A Systematic Review.Int J Environ Res Public Health. 2020 Jul 9;17(14):4955. doi: 10.3390/ijerph17144955. Int J Environ Res Public Health. 2020. PMID: 32660146 Free PMC article.
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA: a Cancer Journal for Clinicians. 2010;60(5):277–300. - PubMed
-
- Riall TS, Nealon WH, Goodwin JS, et al. Pancreatic cancer in the general population: Improvements in survival over the last decade. Journal of Gastrointestinal Surgery. 2006;10(9):1212–1223. - PubMed
-
- Jemal A, Clegg LX, Ward E, et al. Annual report to the nation on the status of cancer, 1975–2001, with a special feature regarding survival. Cancer. 2004;101(1):3–27. - PubMed
-
- Labori KJ, Hjermstad MJ, Wester T, Buanes T, Loge JH. Symptom profiles and palliative care in advanced pancreatic cancer: a prospective study. Supportive Care in Cancer. 2006;14(11):1126–1133. - PubMed
-
- Nieveen van Dijkum EJ, Kuhlmann KF, Terwee CB, Obertop H, de Haes JC, Gouma DJ. Quality of life after curative or palliative surgical treatment of pancreatic and periampullary carcinoma. British Journal of Surgery. 2005;92(4):471–477. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
