

Motor callosal disconnection in early relapsing-remitting multiple sclerosis
- PMID: 21495114
- PMCID: PMC6350254
- DOI: 10.1002/hbm.21071
Motor callosal disconnection in early relapsing-remitting multiple sclerosis
Abstract
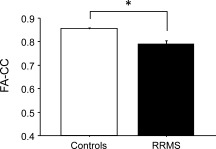
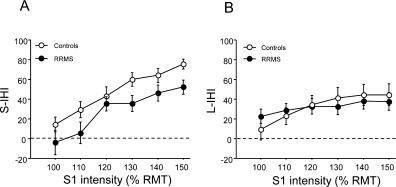
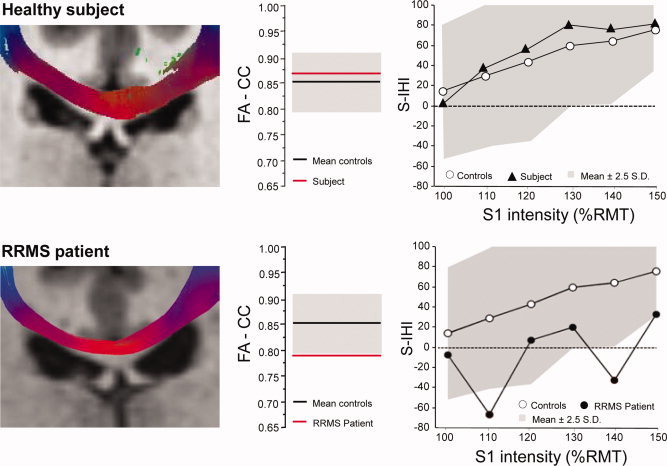
In relapsing-remitting multiple sclerosis (RRMS) the corpus callosum (CC) is often and early affected by macroscopic lesions when investigated by conventional MRI. We sought to determine to which extent microstructural and effective disconnection of the CC are already present in RRMS patients at the earliest stages of the disease prior to evidence of macroscopic CC lesion. We compared 16 very early RRMS patients (median expanded disability status scale (EDSS), 1.5; range, 0-2.0) to an age-matched group of healthy controls and focused analysis to the motor CC, i.e. that part of the CC relaying interhemispheric motor information. A combined functional magnetic resonance imaging/diffusion tensor imaging fiber-tracking procedure was applied to identify the callosal motor fibers (CMFs) connecting the hand areas of the primary motor cortices of the two hemispheres. Fractional anisotropy (FA) within the motor CC (FA-CC) assessed the CMF microstructural integrity. Bifocal paired transcranial magnetic stimulation (TMS) tested short-interval interhemispheric inhibition (S-IHI), an established measure of CMF effective connectivity. FA-CC and S-IHI were significantly reduced in early RRMS compared to healthy controls. Furthermore, a significant linear correlation between microstructure (FA-CC) and function (S-IHI) in the controls was broken down in the patients. These abnormalities were obtained in the absence of macroscopic CMF lesion in conventional MRI, and whilst motor hand/arm function in the nine-hole-peg test and corticospinal conduction time were normal. Findings suggest that reductions in FA and S-IHI may serve as surrogate markers of motor callosal disconnection at the earliest stages of RRMS prior to development of macroscopic lesion.
Copyright © 2010 Wiley-Liss, Inc.
Figures

Similar articles
-
Callosal anatomical and effective connectivity between primary motor cortices predicts visually cued bimanual temporal coordination performance.Brain Struct Funct. 2016 Sep;221(7):3427-43. doi: 10.1007/s00429-015-1110-z. Epub 2015 Sep 13. Brain Struct Funct. 2016. PMID: 26365504
-
The relationship between regional microstructural abnormalities of the corpus callosum and physical and cognitive disability in relapsing-remitting multiple sclerosis.Neuroimage Clin. 2014 Nov 18;7:28-33. doi: 10.1016/j.nicl.2014.11.008. eCollection 2015. Neuroimage Clin. 2014. PMID: 25610764 Free PMC article.
-
Multimodal assessment of normal-appearing corpus callosum is a useful marker of disability in relapsing-remitting multiple sclerosis: an MRI cluster analysis study.J Neurol. 2018 Oct;265(10):2243-2250. doi: 10.1007/s00415-018-8980-y. Epub 2018 Jul 26. J Neurol. 2018. PMID: 30051273
-
Segmented corpus callosum diffusivity correlates with the Expanded Disability Status Scale score in the early stages of relapsing-remitting multiple sclerosis.Clinics (Sao Paulo). 2013;68(8):1115-20. doi: 10.6061/clinics/2013(08)09. Clinics (Sao Paulo). 2013. PMID: 24037007 Free PMC article.
-
Quantitative evaluation of callosal abnormalities in relapsing-remitting multiple sclerosis using diffusion tensor imaging: A systemic review and meta-analysis.Clin Neurol Neurosurg. 2021 Feb;201:106442. doi: 10.1016/j.clineuro.2020.106442. Epub 2020 Dec 24. Clin Neurol Neurosurg. 2021. PMID: 33373835
Cited by
-
Transcranial Magnetic Stimulation as a Potential Biomarker in Multiple Sclerosis: A Systematic Review with Recommendations for Future Research.Neural Plast. 2019 Sep 16;2019:6430596. doi: 10.1155/2019/6430596. eCollection 2019. Neural Plast. 2019. PMID: 31636661 Free PMC article.
-
Bridging the callosal gap in gait: corpus callosum white matter integrity's role in lower limb coordination.Brain Imaging Behav. 2022 Aug;16(4):1552-1562. doi: 10.1007/s11682-021-00612-7. Epub 2022 Jan 28. Brain Imaging Behav. 2022. PMID: 35088352
-
Biomarkers in Multiple Sclerosis: An Up-to-Date Overview.Mult Scler Int. 2013;2013:340508. doi: 10.1155/2013/340508. Epub 2013 Jan 22. Mult Scler Int. 2013. PMID: 23401777 Free PMC article.
-
Interhemispheric inhibition and gait adaptation associations in people with multiple sclerosis.Exp Brain Res. 2024 Jul;242(7):1761-1772. doi: 10.1007/s00221-024-06860-5. Epub 2024 Jun 1. Exp Brain Res. 2024. PMID: 38822825
-
Influence of corpus callosum damage on cognition and physical disability in multiple sclerosis: a multimodal study.PLoS One. 2012;7(5):e37167. doi: 10.1371/journal.pone.0037167. Epub 2012 May 14. PLoS One. 2012. PMID: 22606347 Free PMC article.
References
-
- Aboitiz F, Scheibel AB, Fisher RS, Zaidel E ( 1992): Fiber composition of the human corpus callosum. Brain Res 598: 143–153. - PubMed
-
- Alexander AL, Hasan K, Kindlmann G, Parker DL, Tsuruda JS ( 2000): A geometric analysis of diffusion tensor measurements of the human brain. Magn Reson Med 44: 283–291. - PubMed
-
- Bammer R, Augustin M, Strasser‐Fuchs S, Seifert T, Kapeller P, Stollberger R, Ebner F, Hartung HP, Fazekas F ( 2000): Magnetic resonance diffusion tensor imaging for characterizing diffuse and focal white matter abnormalities in multiple sclerosis. Magn Reson Med 44: 583–591. - PubMed
-
- Beaulieu C ( 2002): The basis of anisotropic water diffusion in the nervous system—A technical review. NMR Biomed 15: 435–455. - PubMed
-
- Bester M, Heesen C, Schippling S, Martin R, Ding XQ, Holst B, Fiehler J ( 2008): Early anisotropy changes in the corpus callosum of patients with optic neuritis. Neuroradiology 50: 549–557. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
