

Minimal disease assessment in the treatment of children and adolescents with intermediate-risk (Stage III/IV) B-cell non-Hodgkin lymphoma: a children's oncology group report
- PMID: 21496005
- PMCID: PMC3103617
- DOI: 10.1111/j.1365-2141.2011.08681.x
Minimal disease assessment in the treatment of children and adolescents with intermediate-risk (Stage III/IV) B-cell non-Hodgkin lymphoma: a children's oncology group report
Abstract
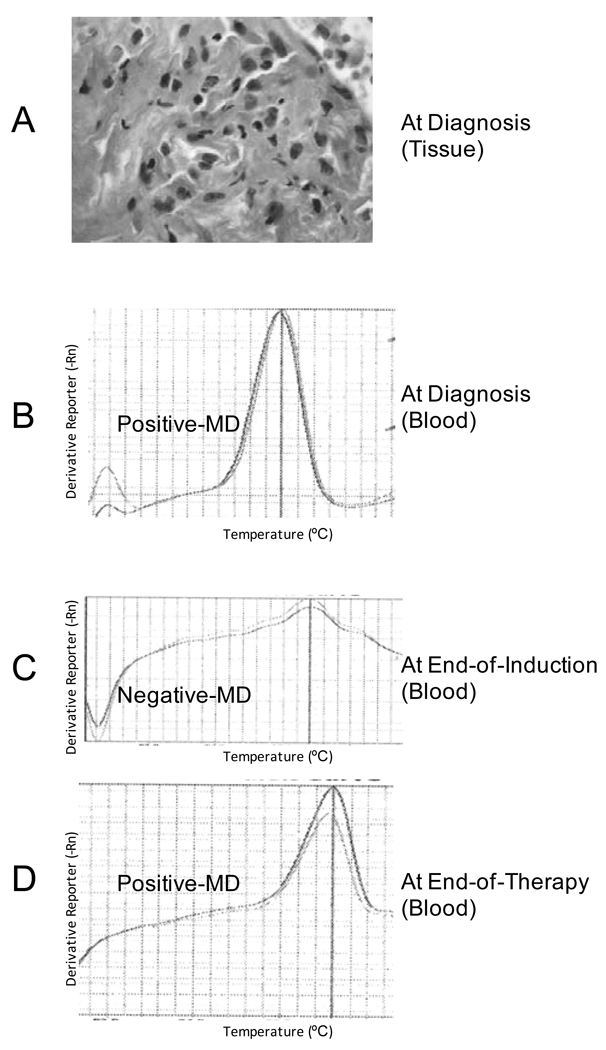
Children/adolescents with mature B-cell non-Hodgkin lymphoma (B-NHL) have an excellent prognosis but relapses still occur. While chromosomal aberrations and/or clonal immunoglobulin (Ig) gene rearrangements may indicate risk of failure, a more universal approach was developed to detect minimal disease (MD). Children/adolescents with intermediate-risk B-NHL were treated with French-British-American/Lymphome Malins de Burkitt 96 (FAB/LMB96) B4 modified chemotherapy and rituximab. Specimens from diagnosis, end of induction (EOI), and end of therapy (EOT) were assayed for MD. Initial specimens were screened for IGHV family usage with primer pools followed by individual primers to identify MD. Thirty-two diagnostic/staging specimens screened positive with primer pools and unique IGHV family primers were identified. Two patients relapsed; first relapse (4 months from diagnosis) was MD-positive at EOI, the second (36 months from diagnosis) was MD-positive at EOT. At EOI, recurrent rates were similar between the MRD-positive and MRD-negative patients (P = 0·40). At EOT, only 13/32 patients had MRD data available with one relapse in the MRD-positive group and no recurrences in the MRD-negative group (P = 0·077). The study demonstrated molecular-disseminated disease in which IgIGHV primer pools could be used to assess MD. This feasibility study supports future investigations to assess the validity and significance of MD screening in a larger cohort of patients with intermediate-risk mature B-NHL.
© 2011 Blackwell Publishing Ltd.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURE: T.G. is on the scientific advisory board for Roche. All other authors declare no conflict of interest.
Figures

References
-
- Bruggemann M, Schrauder A, Raff T, Pfeifer H, Dworzak M, Ottmann OG, Asnafi V, Baruchel A, Bassan R, Benoit Y, Biondi A, Cave H, Dombret H, Fielding AK, Foa R, Gokbuget N, Goldstone AH, Goulden N, Henze G, Hoelzer D, Janka-Schaub GE, Macintyre EA, Pieters R, Rambaldi A, Ribera JM, Schmiegelow K, Spinelli O, Stary J, von Stackelberg A, Kneba M, Schrappe M, van Dongen JJ. Standardized MRD quantification in European ALL trials: proceedings of the Second International Symposium on MRD assessment in Kiel, Germany, 18-20 September 2008. Leukemia. 2010;24:521–535. - PubMed
-
- Cairo MS, Gerrard M, Sposto R, Auperin A, Pinkerton CR, Michon J, Weston C, Perkins SL, Raphael M, McCarthy K, Patte C. Results of a randomized international study of high-risk central nervous system B non-Hodgkin lymphoma and B acute lymphoblastic leukemia in children and adolescents. Blood. 2007;109:2736–2743. - PMC - PubMed
-
- Cairo M, Lynch J, Harrison L, Van de Ven C, Gross T, Shiramizu B, Sanger W, Perkins S, Goldman S. Safety, efficacy and rituximab levels following chemoimmunotherapy (rituximab + FAB chemotherapy) in children and adolescents with mature B-cell non-Hodgkin lymphoma (B-NHL): a Children’s Oncology Group report. Blood (ASH meeting abstracts) 2008;112:838a.
-
- Cairo MS, Lynch JC, Harrison L, Perkins SL, Shiramizu B, Gross TG, Sanger W, Goldman S. Safety, kinetics, and outcome following rituximab (R) in combination with FAB chemotherapy in children and adolescents (C+A) with stage III/IV (Group B) and BM+/CNS+ (Group C) mature B-NHL: A Children's Oncology Group report. J Clin Oncol (Meeting Abstracts) 2010;28 9536-.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
