

Anti-fibrogenic strategies and the regression of fibrosis
- PMID: 21497747
- PMCID: PMC3086317
- DOI: 10.1016/j.bpg.2011.02.011
Anti-fibrogenic strategies and the regression of fibrosis
Abstract
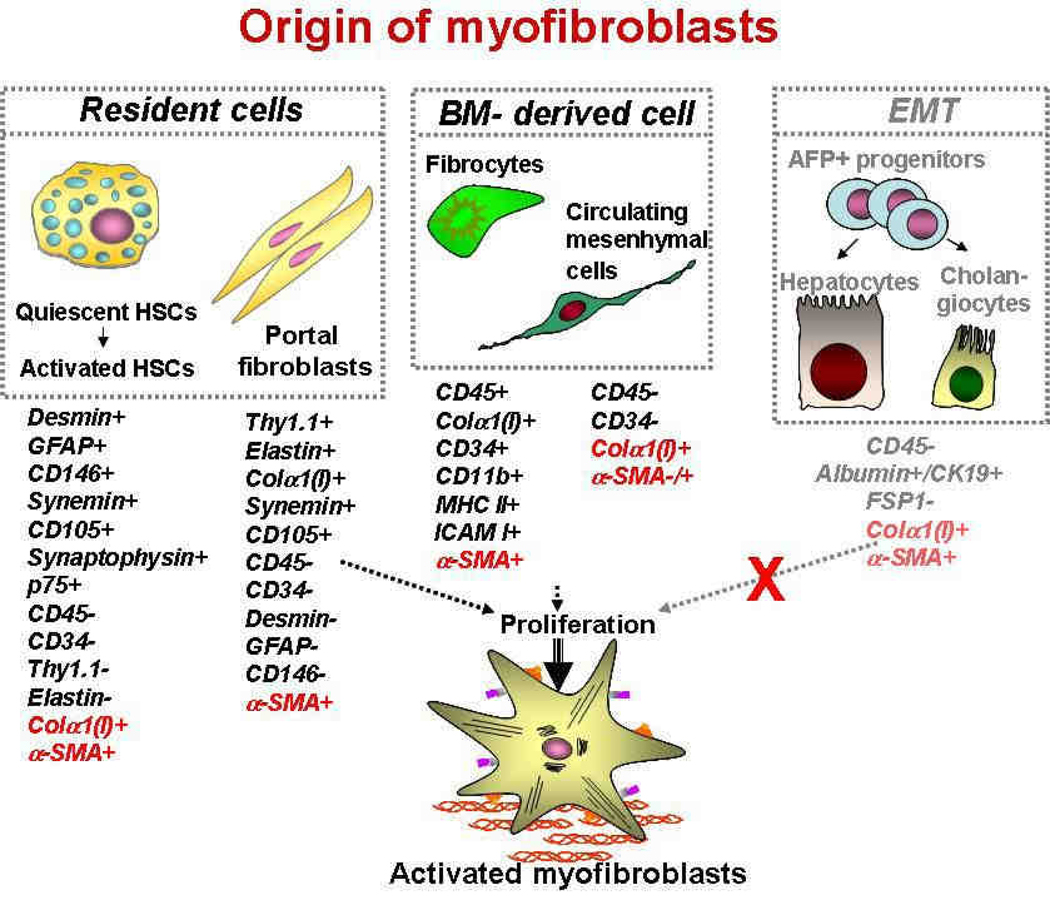
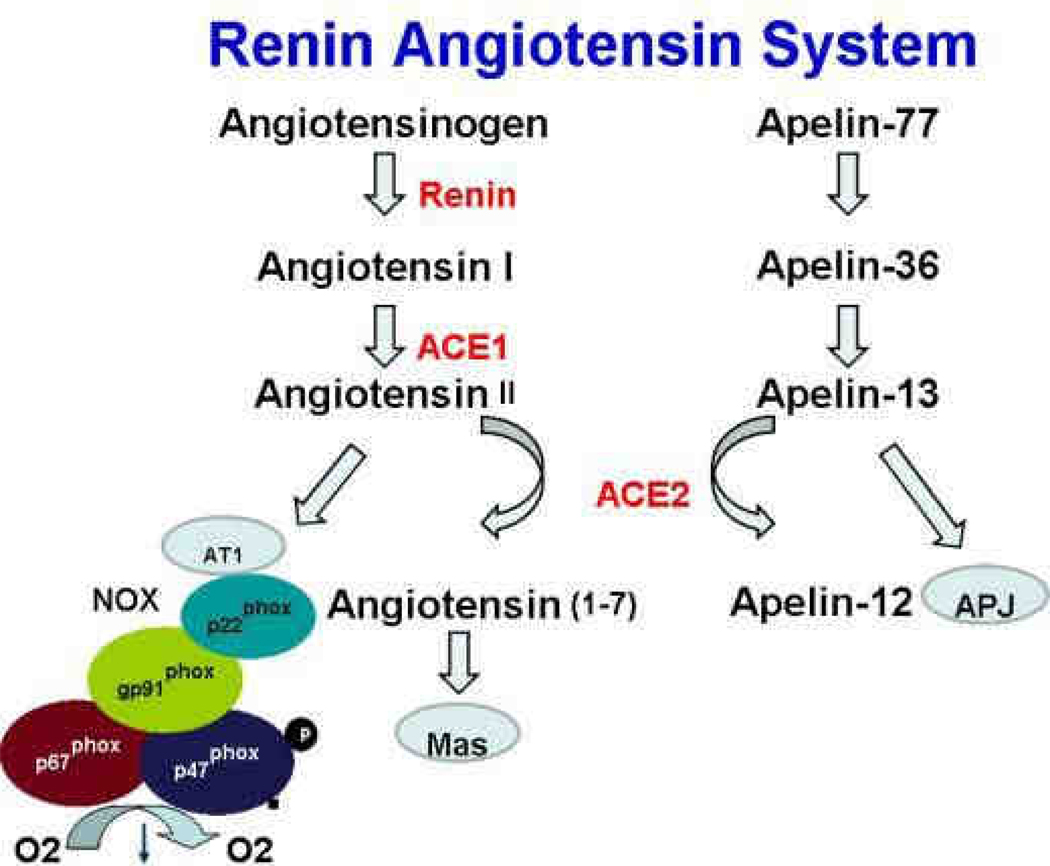
Liver fibrosis is an outcome of many chronic diseases, and often results in cirrhosis, liver failure, and portal hypertension. Liver transplantation is the only treatment available for patients with advanced stage of fibrosis. Therefore, alternative methods are required to develop new strategies for anti-fibrotic therapy. Available treatments are designed to substitute for liver transplantation or bridge the patients, they include inhibitors of fibrogenic cytokines such as TGF-β1 and EGF, inhibitors of rennin angiotensin system, and blockers of TLR4 signalling. Development of liver fibrosis is orchestrated by many cell types. However, activated myofibroblasts remain the primary target for anti-fibrotic therapy. Hepatic stellate cells and portal fibroblasts are considered to play a major role in development of liver fibrosis. Here we discuss the origin of activated myofibroblasts and different aspects of their activation, differentiation and potential inactivation during regression of liver fibrosis.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Conflict of interest statement
No conflict of interest has been declared by the authors.
Figures
References
-
- Kisseleva T, Brenner DA. Hepatic stellate cells and the reversal of fibrosis. J Gastroenterol Hepatol. 2006;21 Suppl 3:S84–S87. - PubMed
-
- Gomperts BN, Strieter RM. Fibrocytes in lung disease. J Leukoc Biol. 2007;82:449–456. - PubMed
-
- Fallowfield JA, Mizuno M, Kendall TJ, et al. Scar-associated macrophages are a major source of hepatic matrix metalloproteinase-13 and facilitate the resolution of murine hepatic fibrosis. J Immunol. 2007;178:5288–5295. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
