

Society of Thoracic Surgeons Risk Score predicts hospital charges and resource use after aortic valve replacement
- PMID: 21497834
- PMCID: PMC3156832
- DOI: 10.1016/j.jtcvs.2011.02.038
Society of Thoracic Surgeons Risk Score predicts hospital charges and resource use after aortic valve replacement
Abstract
Objective: The impact of Society of Thoracic Surgeons predicted mortality risk score on resource use has not been previously studied. We hypothesize that increasing Society of Thoracic Surgeons risk scores in patients undergoing aortic valve replacement are associated with greater hospital charges.
Methods: Clinical and financial data for patients undergoing aortic valve replacement at The Johns Hopkins Hospital over a 10-year period (January 2000 to December 2009) were reviewed. The current Society of Thoracic Surgeons formula (v2.61) for in-hospital mortality was used for all patients. After stratification into risk quartiles, index admission hospital charges were compared across risk strata with rank-sum and Kruskal-Wallis tests. Linear regression and Spearman's coefficient assessed correlation and goodness of fit. Multivariable analysis assessed relative contributions of individual variables on overall charges.
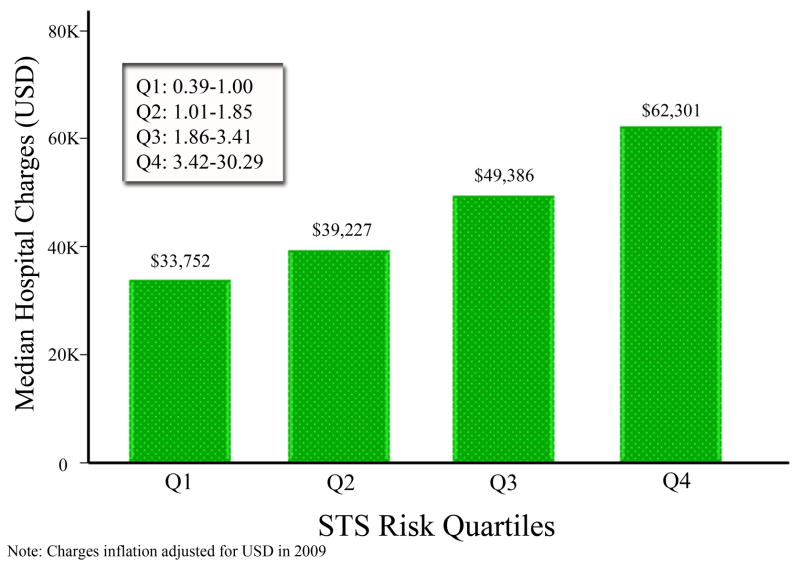
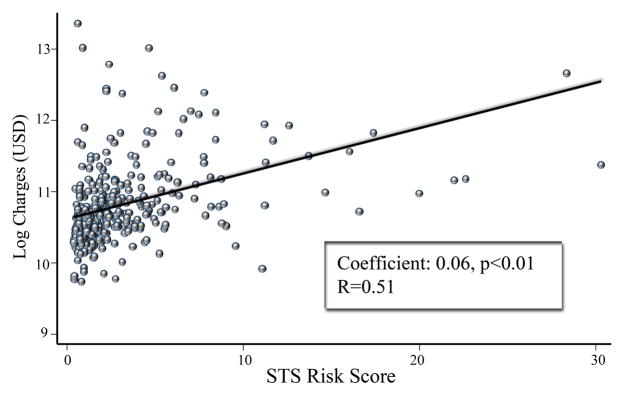
Results: A total of 553 patients underwent aortic valve replacement during the study period. Average predicted mortality was 2.9% (±3.4) and actual mortality was 3.4% for aortic valve replacement. Median charges were greater in the upper quartile of patients undergoing aortic valve replacement (quartiles 1-3, $39,949 [interquartile range, 32,708-51,323] vs quartile 4, $62,301 [interquartile range, 45,952-97,103], P < .01]. On univariate linear regression, there was a positive correlation between Society of Thoracic Surgeons risk score and log-transformed charges (coefficient, 0.06; 95% confidence interval, 0.05-0.07; P < .01). Spearman's correlation R-value was 0.51. This positive correlation persisted in risk-adjusted multivariable linear regression. Each 1% increase in Society of Thoracic Surgeons risk score was associated with an added $3000 in hospital charges.
Conclusions: This is the first study to show that increasing Society of Thoracic Surgeons risk score predicts greater charges after aortic valve replacement. As competing therapies, such as percutaneous valve replacement, emerge to treat high-risk patients, these results serve as a benchmark to compare resource use.
Copyright © 2011 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Society of Thoracic Surgeons 2008 cardiac risk models predict in-hospital mortality of heart valve surgery in a Chinese population: a multicenter study.J Thorac Cardiovasc Surg. 2014 Dec;148(6):3036-41. doi: 10.1016/j.jtcvs.2013.09.081. Epub 2014 Jul 10. J Thorac Cardiovasc Surg. 2014. PMID: 25091531
-
Patients at low surgical risk as defined by the Society of Thoracic Surgeons Score undergoing isolated interventional or surgical aortic valve implantation: in-hospital data and 1-year results from the German Aortic Valve Registry (GARY).Eur Heart J. 2019 May 1;40(17):1323-1330. doi: 10.1093/eurheartj/ehy699. Eur Heart J. 2019. PMID: 30445543
-
Performance of EuroSCORE II and Society of Thoracic Surgeons risk scores in elderly patients undergoing aortic valve replacement surgery.Arch Cardiovasc Dis. 2021 Jun-Jul;114(6-7):474-481. doi: 10.1016/j.acvd.2020.12.004. Epub 2021 Feb 6. Arch Cardiovasc Dis. 2021. PMID: 33558164
-
Meta-analysis on the performance of the EuroSCORE II and the Society of Thoracic Surgeons Scores in patients undergoing aortic valve replacement.J Cardiothorac Vasc Anesth. 2014 Dec;28(6):1533-9. doi: 10.1053/j.jvca.2014.03.014. Epub 2014 Sep 26. J Cardiothorac Vasc Anesth. 2014. PMID: 25263775
-
A comprehensive review of the PARTNER trial.J Thorac Cardiovasc Surg. 2013 Mar;145(3 Suppl):S11-6. doi: 10.1016/j.jtcvs.2012.11.051. J Thorac Cardiovasc Surg. 2013. PMID: 23410766 Review.
Cited by
-
The use of correlation functions in thoracic surgery research.J Thorac Dis. 2015 Mar;7(3):E11-5. doi: 10.3978/j.issn.2072-1439.2015.01.54. J Thorac Dis. 2015. PMID: 25922740 Free PMC article. No abstract available.
-
Comparison of EuroSCORE II and STS Risk Scoring Systems in Patients who Underwent Open-heart Surgery.Turk J Anaesthesiol Reanim. 2025 Jul 24;53(4):163-169. doi: 10.4274/TJAR.2025.241778. Epub 2025 Jul 9. Turk J Anaesthesiol Reanim. 2025. PMID: 40631722 Free PMC article.
-
Factors Associated With High Resource Use in Elective Adult Cardiac Surgery From 2005 to 2016.Ann Thorac Surg. 2022 Jan;113(1):58-65. doi: 10.1016/j.athoracsur.2021.02.059. Epub 2021 Mar 6. Ann Thorac Surg. 2022. PMID: 33689737 Free PMC article.
-
Performance of scoring systems for predicting mortality after cardiac surgery in the elderly.Arch Peru Cardiol Cir Cardiovasc. 2025 Feb 12;6(1):29-35. doi: 10.47487/apcyccv.v6i1.459. eCollection 2025 Jan-Mar. Arch Peru Cardiol Cir Cardiovasc. 2025. PMID: 40376122 Free PMC article.
-
General and acute care surgical procedures in patients with left ventricular assist devices.World J Surg. 2014 Apr;38(4):765-73. doi: 10.1007/s00268-013-2403-0. World J Surg. 2014. PMID: 24357244
References
-
- Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–1607. - PubMed
-
- Ross J, Jr, Braunwald E. Aortic stenosis. Circulation. 1968;38:61–67. - PubMed
-
- Elbardissi AW, Shekar P, Couper GS, Cohn LH. Minimally invasive aortic valve replacement in octogenarian, high-risk, transcatheter aortic valve implantation candidates. J Thorac Cardiovasc Surg. 2011;141:328–335. - PubMed
-
- Schwarz F, Baumann P, Manthey J, Hoffmann M, Schuler G, Mehmel HC, et al. The effect of aortic valve replacement on survival. Circulation. 1982;66:1105–1110. - PubMed
-
- Varadarajan P, Kapoor N, Bansal RC, Pai RG. Survival in elderly patients with severe aortic stenosis is dramatically improved by aortic valve replacement: Results from a cohort of 277 patients aged > or =80 years. Eur J Cardiothorac Surg. 2006;30:722–727. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
