

Relationship between hyperglycemia and outcome in children with severe traumatic brain injury
- PMID: 21499170
- PMCID: PMC3677026
- DOI: 10.1097/PCC.0b013e3182192c30
Relationship between hyperglycemia and outcome in children with severe traumatic brain injury
Abstract
Objective: To determine the relationship between hyperglycemia and outcome in infants and children after severe traumatic brain injury.
Design: Retrospective review of a prospectively collected Pediatric Neurotrauma Registry.
Setting and patients: Children admitted after severe traumatic brain injury (postresuscitation Glasgow Coma Scale ≤ 8) were studied (1999-2004). A subset of children (n = 28) were concurrently enrolled in a randomized, controlled clinical trial of early hypothermia for neuroprotection.
Interventions: Demographic data, serum glucose concentrations, and outcome assessments were collected.
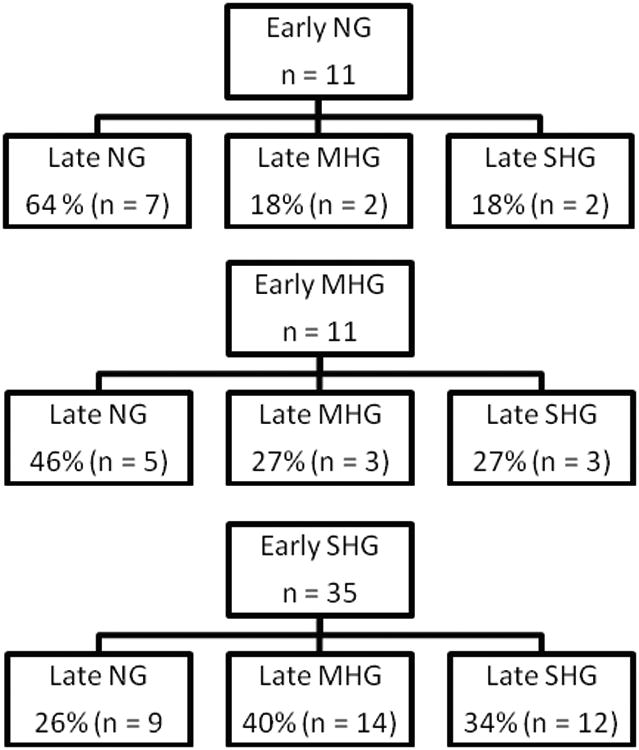
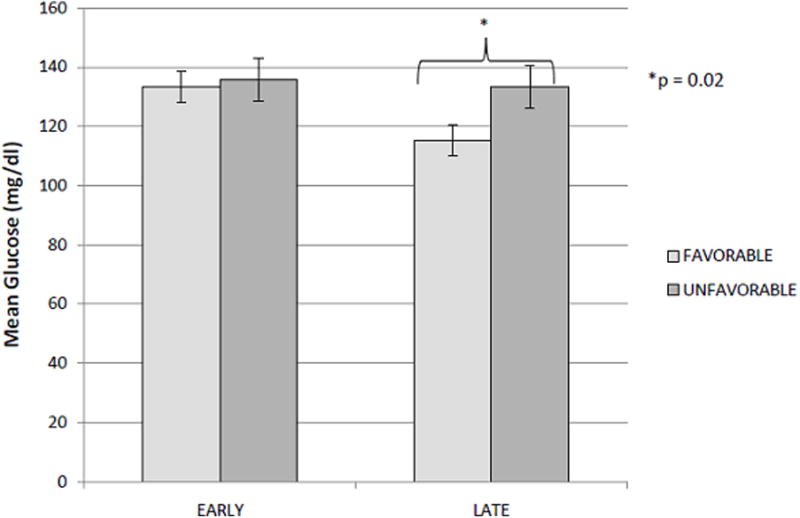
Methods and main results: Children (n = 57) were treated with a standard traumatic brain injury protocol. Exogenous glucose was withheld for 48 hrs after injury unless hypoglycemia was observed (blood glucose <70 mg/dL). Early (first 48 hrs) and Late (49-168 hrs) time periods were defined and mean blood glucose concentrations were calculated. Additionally, children were categorized based on peak blood glucose concentrations during each time period (normal, blood glucose <150 mg/dL; mild hyperglycemia, blood glucose ≤ 200 mg/dL; severe hyperglycemia, blood glucose >200 mg/dL). In the Late period, an association between elevated mean serum glucose concentration and outcome was observed (133.5 ± 5.6 mg/dL in the unfavorable group vs. 115.4 ± 4.1 mg/dL in favorable group, p = .02). This association continued to be significant after correcting for injury severity, age, and exposure to insulin (p = .03). Similarly, in the Late period, children within the severe hyperglycemia group had decreased incidence of good outcome compared to children within the other glycemic groups (% good outcome: normal, 61.9%; mild hyperglycemia, 73.7%; severe hyperglycemia, 33.3%; p = .05). However, when adjusted for exposure to insulin, this relationship was no longer statistically significant.
Conclusions: In children with severe traumatic brain injury, hyperglycemia beyond the initial 48 hrs is associated with poor outcome. This relationship was observed in both our analysis of mean blood glucose concentrations as well as among the patients with episodic severe hyperglycemia. This observation suggests a relationship between hyperglycemia and outcome from traumatic brain injury. However, only a prospective study can answer the important question of whether manipulating serum glucose concentration can improve outcome after traumatic brain injury in children.
Figures

References
-
- Yates AR, Dyke PC, 2nd, Taeed R, et al. Hyperglycemia is a marker for poor outcome in the postoperative pediatric cardiac patient. Pediatr Crit Care Med. 2006;7(4):351–355. - PubMed
-
- Hirshberg E, Larsen G, Van Duker H. Alterations in glucose homeostasis in the pediatric intensive care unit: Hyperglycemia and glucose variability are associated with increased mortality and morbidity. Pediatr Crit Care Med. 2008;9(4):361–366. - PubMed
-
- Yung M, Wilkins B, Norton L, et al. Glucose control, organ failure, and mortality in pediatric intensive care. Pediatr Crit Care Med. 2008;9(2):147–152. - PubMed
-
- Ulate KP, Lima Falcao GC, Bielefeld MR, et al. Strict glycemic targets need not be so strict: a more permissive glycemic range for critically ill children. Pediatrics. 2008;122(4):e898–904. - PubMed
-
- Preissig CM, Rigby MR, Maher KO. Glycemic control for postoperative pediatric cardiac patients. Pediatr Cardiol. 2009;30(8):1098–1104. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
