

Neonatal resuscitation and immediate newborn assessment and stimulation for the prevention of neonatal deaths: a systematic review, meta-analysis and Delphi estimation of mortality effect
- PMID: 21501429
- PMCID: PMC3231885
- DOI: 10.1186/1471-2458-11-S3-S12
Neonatal resuscitation and immediate newborn assessment and stimulation for the prevention of neonatal deaths: a systematic review, meta-analysis and Delphi estimation of mortality effect
Abstract
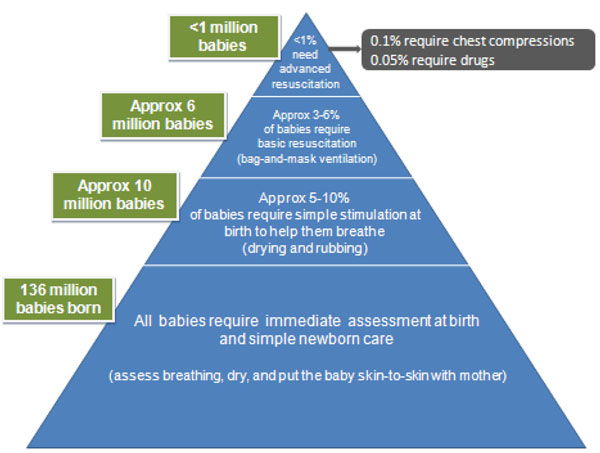
Background: Of 136 million babies born annually, around 10 million require assistance to breathe. Each year 814,000 neonatal deaths result from intrapartum-related events in term babies (previously "birth asphyxia") and 1.03 million from complications of prematurity. No systematic assessment of mortality reduction from tactile stimulation or resuscitation has been published.
Objective: To estimate the mortality effect of immediate newborn assessment and stimulation, and basic resuscitation on neonatal deaths due to term intrapartum-related events or preterm birth, for facility and home births.
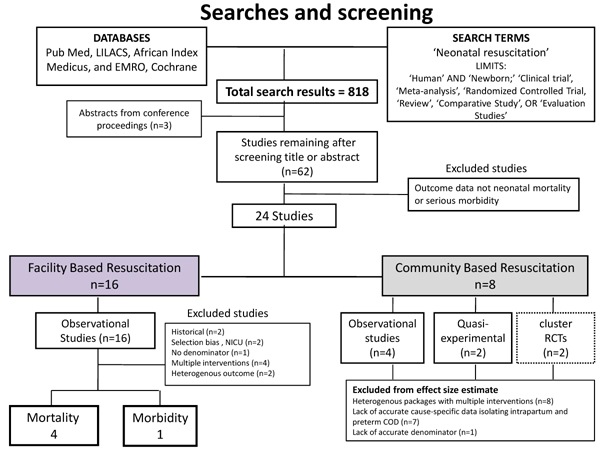
Methods: We conducted systematic reviews for studies reporting relevant mortality or morbidity outcomes. Evidence was assessed using GRADE criteria adapted to provide a systematic approach to mortality effect estimates for the Lives Saved Tool (LiST). Meta-analysis was performed if appropriate. For interventions with low quality evidence but strong recommendation for implementation, a Delphi panel was convened to estimate effect size.
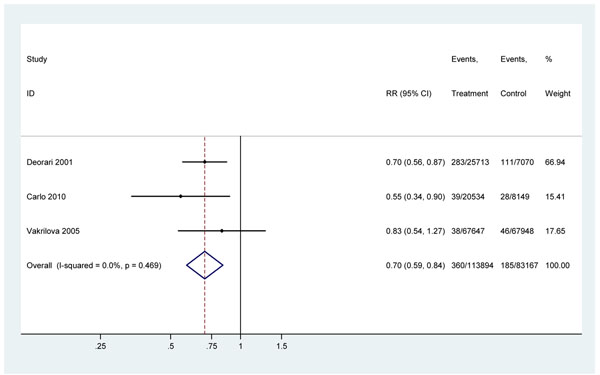
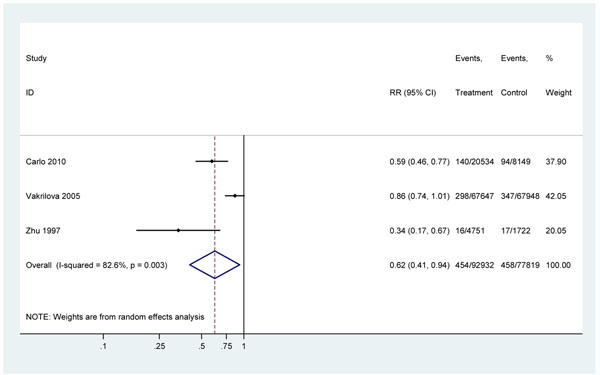
Results: We identified 24 studies of neonatal resuscitation reporting mortality outcomes (20 observational, 2 quasi-experimental, 2 cluster randomized controlled trials), but none of immediate newborn assessment and stimulation alone. A meta-analysis of three facility-based studies examined the effect of resuscitation training on intrapartum-related neonatal deaths (RR= 0.70, 95%CI 0.59-0.84); this estimate was used for the effect of facility-based basic neonatal resuscitation (additional to stimulation). The evidence for preterm mortality effect was low quality and thus expert opinion was sought. In community-based studies, resuscitation training was part of packages with multiple concurrent interventions, and/or studies did not distinguish term intrapartum-related from preterm deaths, hence no meta-analysis was conducted. Our Delphi panel of 18 experts estimated that immediate newborn assessment and stimulation would reduce both intrapartum-related and preterm deaths by 10%, facility-based resuscitation would prevent a further 10% of preterm deaths, and community-based resuscitation would prevent further 20% of intrapartum-related and 5% of preterm deaths.
Conclusion: Neonatal resuscitation training in facilities reduces term intrapartum-related deaths by 30%. Yet, coverage of this intervention remains low in countries where most neonatal deaths occur and is a missed opportunity to save lives. Expert opinion supports smaller effects of neonatal resuscitation on preterm mortality in facilities and of basic resuscitation and newborn assessment and stimulation at community level. Further evaluation is required for impact, cost and implementation strategies in various contexts.
Funding: This work was supported by the Bill & Melinda Gates Foundation through a grant to the US Fund for UNICEF, and to the Saving Newborn Lives program of Save the Children, through Save the Children US.
Figures
References
-
- Zhu XY, Fang HQ, Zeng SP, Li YM, Lin HL, Shi SZ. The impact of the neonatal resuscitation program guidelines (NRPG) on the neonatal mortality in a hospital in Zhuhai, China. Singapore Med J. 1997;38(11):485–487. - PubMed
-
- Organization WH. The World Health Report 2005- make every mother and child count. Geneva, Switzerland: World Health Organization; 2005.
-
- Bang AT, Bang RA, Baitule SB, Reddy HM, Deshmukh MD. Management of birth asphyxia in home deliveries in rural Gadchiroli: the effect of two types of birth attendants and of resuscitating with mouth-to-mouth, tube-mask or bag-mask. J Perinatol. 2005;25(Suppl 1):S82–91. doi: 10.1038/sj.jp.7211275. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
