

Effectiveness of interventions to screen and manage infections during pregnancy on reducing stillbirths: a review
- PMID: 21501448
- PMCID: PMC3231903
- DOI: 10.1186/1471-2458-11-S3-S3
Effectiveness of interventions to screen and manage infections during pregnancy on reducing stillbirths: a review
Abstract
Background: Infection is a well acknowledged cause of stillbirths and may account for about half of all perinatal deaths today, especially in developing countries. This review presents the impact of interventions targeting various important infections during pregnancy on stillbirth or perinatal mortality.
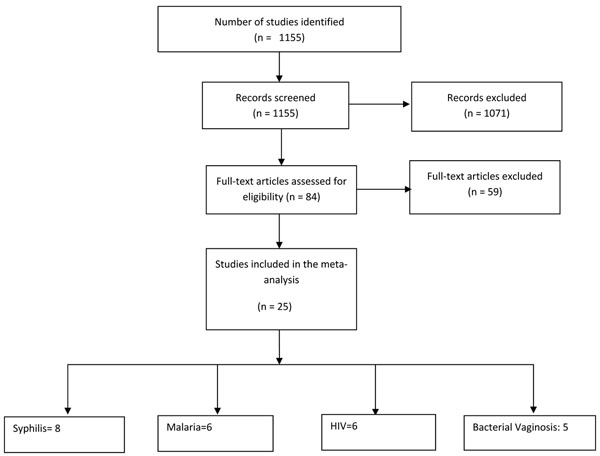
Methods: We undertook a systematic review including all relevant literature on interventions dealing with infections during pregnancy for assessment of effects on stillbirths or perinatal mortality. The quality of the evidence was assessed using the adapted Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach by Child Health Epidemiology Reference Group (CHERG). For the outcome of interest, namely stillbirth, we applied the rules developed by CHERG to recommend a final estimate for reduction in stillbirth for input to the Lives Saved Tool (LiST) model.
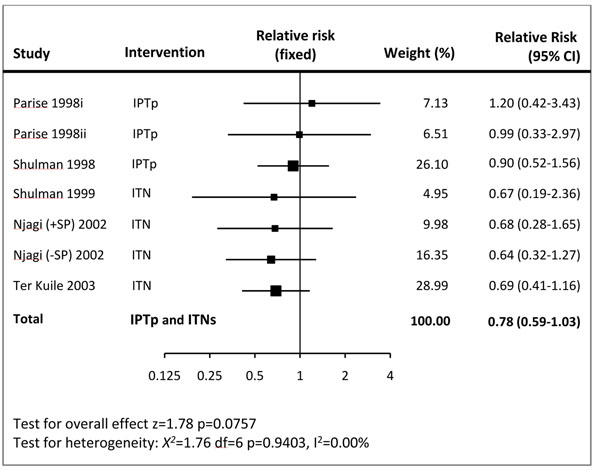
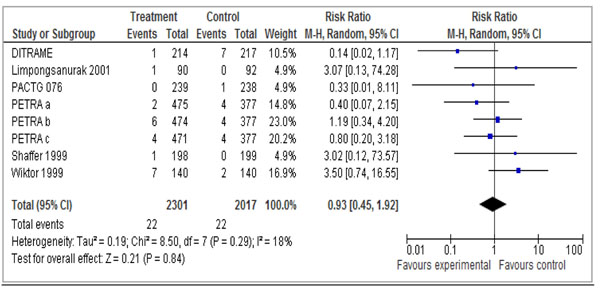
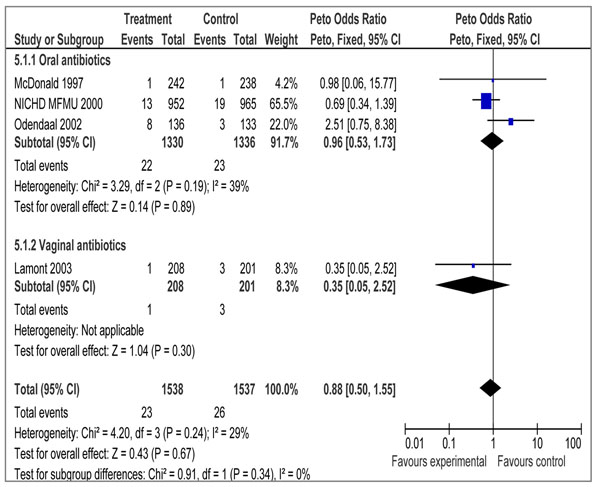
Results: A total of 25 studies were included in the review. A random-effects meta-analysis of observational studies of detection and treatment of syphilis during pregnancy showed a significant 80% reduction in stillbirths [Relative risk (RR) = 0.20; 95% confidence interval (CI): 0.12 - 0.34) that is recommended for inclusion in the LiST model. Our meta-analysis showed the malaria prevention interventions i.e. intermittent preventive treatment (IPTp) and insecticide-treated mosquito nets (ITNs) can reduce stillbirths by 22%, however results were not statistically significant (RR = 0.78; 95% CI: 0.59 - 1.03). For human immunodeficiency virus infection, a pooled analysis of 6 randomized controlled trials (RCTs) failed to show a statistically significant reduction in stillbirth with the use of antiretroviral in pregnancy compared to placebo (RR = 0.93; 95% CI: 0.45 - 1.92). Similarly, pooled analysis combining four studies for the treatment of bacterial vaginosis (3 for oral and 1 for vaginal antibiotic) failed to yield a significant impact on perinatal mortality (OR = 0.88; 95% CI: 0.50 - 1.55).
Conclusions: The clearest evidence of impact in stillbirth reduction was found for adequate prevention and treatment of syphilis infection and possibly malaria. At present, large gaps exist in the growing list of stillbirth risk factors, especially those that are infection related. Potential causes of stillbirths including HIV and TORCH infections need to be investigated further to help establish the role of prevention/treatment and its subsequent impact on stillbirth reduction.
Figures
References
-
- Herschel M, Hsieh HL, Mittendorf R, Khoshnood B, Covert RF, Lee KS. Fetal death in a population of black women. Am J Prev Med. 1995;11(3):185–189. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
