

Valganciclovir reduces T cell activation in HIV-infected individuals with incomplete CD4+ T cell recovery on antiretroviral therapy
- PMID: 21502083
- PMCID: PMC3080892
- DOI: 10.1093/infdis/jir060
Valganciclovir reduces T cell activation in HIV-infected individuals with incomplete CD4+ T cell recovery on antiretroviral therapy
Abstract
Background: Elevated immune activation persists during treated human immunodeficiency virus (HIV) infection and is associated with blunted CD4 recovery and premature mortality, but its causes remain incompletely characterized. We hypothesized that asymptomatic cytomegalovirus (CMV) replication might contribute to immune activation in this setting.
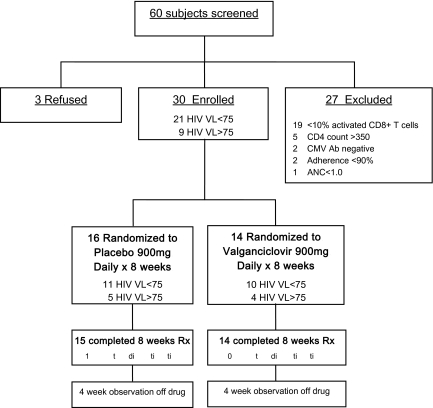
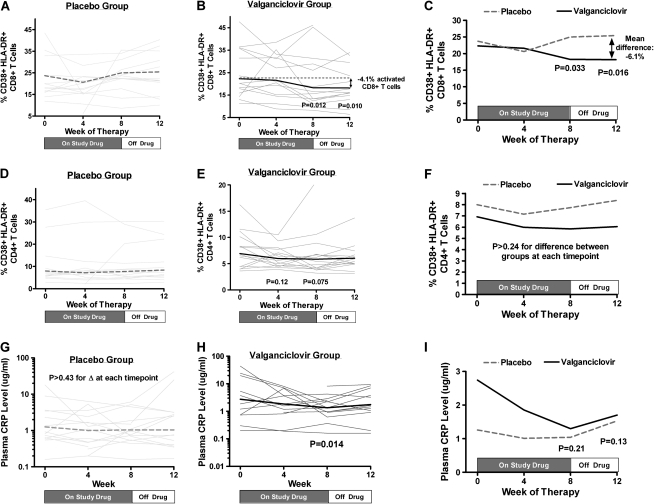
Methods: Thirty antiretroviral therapy-treated HIV-infected CMV-seropositive participants with CD4 counts <350 cells/mm(3) were randomized to receive valganciclovir 900 mg daily or placebo for 8 weeks, followed by an additional 4-week observation period. The primary outcome was the week 8 change in percentage of activated (CD38(+) HLA-DR(+)) CD8(+) T cells.
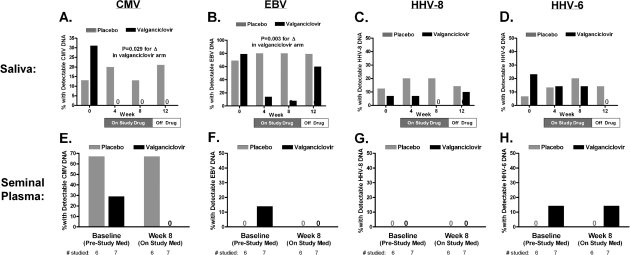
Results: Fourteen participants were randomized to valganciclovir and 16 to placebo. Most participants (21 [70%] of 30) had plasma HIV RNA levels <75 copies/mL. The median CD4 count was 190 (IQR: 134-232) cells/mm(3), and 12 (40%) of 30 had detectable CMV DNA in saliva, plasma, or semen at baseline. CMV DNA continued to be detectable at weeks 4-12 in 7 (44%) of 16 placebo-treated participants, but in none of the valganciclovir-treated participants (P = .007). Valganciclovir-treated participants had significantly greater reductions in CD8 activation at weeks 8 (P = .03) and 12 (P = .02) than did placebo-treated participants. These trends were significant even among those with undetectable plasma HIV RNA levels.
Conclusions: CMV (and/or other herpesvirus) replication is a significant cause of immune activation in HIV-infected individuals with incomplete antiretroviral therapy-mediated CD4(+) T cell recovery.
Clinical trials registration: NCT00264290.
Figures

References
-
- Lohse N, Hansen AB, Pedersen G, et al. Survival of persons with and without HIV infection in Denmark, 1995–2005. Ann Intern Med. 2007;146:87–95. - PubMed
-
- Lewden C, Chene G, Morlat P, et al. HIV-infected adults with a CD4 cell count greater than 500 cells/mm3 on long-term combination antiretroviral therapy reach same mortality rates as the general population. J Acquir Immune Defic Syndr. 2007;46:72–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
