

Outcomes of laparoscopic versus open fundoplication in children's hospitals: 2005-2008
- PMID: 21502226
- PMCID: PMC3387863
- DOI: 10.1542/peds.2010-1198
Outcomes of laparoscopic versus open fundoplication in children's hospitals: 2005-2008
Abstract
Background: Fundoplication is a common pediatric surgery, but little data comparing the laparoscopic approach with the open approach have been published.
Objective: To compare infection rates, complication rates, length of stay, and cost for laparoscopic fundoplication versus open fundoplication among pediatric patients and to examine trends in utilization of laparoscopic fundoplication.
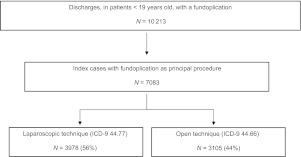
Methods: We used the Pediatric Health Information System database to conduct a retrospective study of children (aged <19 years) admitted for a fundoplication between 2005 and 2008. Descriptive characteristics for those undergoing a laparoscopic and open fundoplication were compared. Multivariate regression with random effects specified at the hospital level was used to model the association between laparoscopic fundoplication and the outcomes.
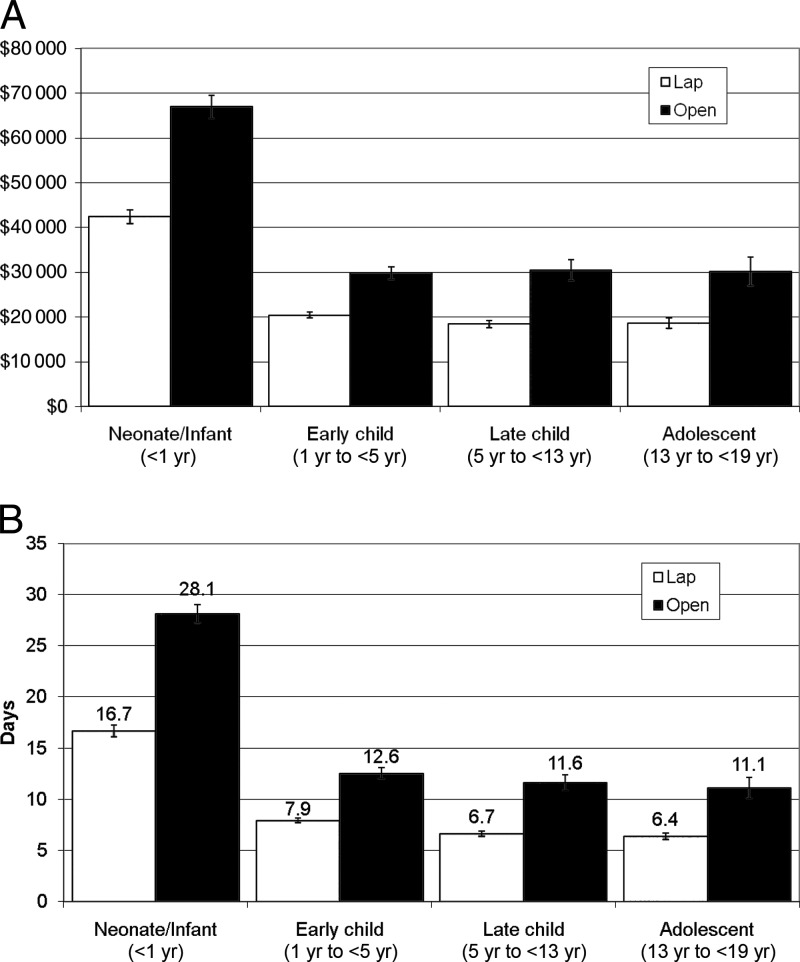
Results: Fifty-six percent of 7083 fundoplication admissions had laparoscopic fundoplication. Median length of stay was 4 days for laparoscopic and 10 days for open fundoplication. The median cost of laparoscopic fundoplication was $13 003 versus $22 487 for open fundoplication. Laparoscopic fundoplication was associated with a 24% and 51% reduction in the adjusted odds of infection and surgical complications, respectively. The proportion of fundoplications performed laparoscopically increased from 51% in 2005 to 63% in 2008 (P < .001), but there was no increase in the overall fundoplication rate.
Conclusions: In a large study of children's hospitals, laparoscopic fundoplication was associated with improved outcomes compared with the open procedure, even after adjustment for patient severity. Laparoscopic fundoplication has become the most common form of antireflux surgery in children over 1 year of age, but this has not been associated with an increase in the overall utilization of the fundoplication procedure. These data have important implications for clinical practice and surgical training.
Figures
References
-
- HCUPnet, Healthcare Cost and Utilization Project 2006 Agency for Healthcare Research and Quality, Rockville, MD: Agency for Healthcare Research and Quality (AHRQ). [serial online] 2008;Accessed January 10, 2010
-
- Diaz DM, Gibbons TE, Heiss K, Wulkan ML, Ricketts RR, Gold BD. Antireflux surgery outcomes in pediatric gastroesophageal reflux disease. Am J Gastroenterol. 2005;100(8):1844–1852 - PubMed
-
- Mattioli G, Repetto P, Carlini C, et al. Laparoscopic vs open approach for the treatment of gastroesophageal reflux in children. Surg Endosc. 2002;16(5):750–752 - PubMed
-
- Somme S, Rodriguez JA, Kirsch DG, Liu DC. Laparoscopic versus open fundoplication in infants. Surg Endosc. 2002;16(1):54–56 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
