

Toxicogenomics of nevirapine-associated cutaneous and hepatic adverse events among populations of African, Asian, and European descent
- PMID: 21505298
- PMCID: PMC3387531
- DOI: 10.1097/QAD.0b013e32834779df
Toxicogenomics of nevirapine-associated cutaneous and hepatic adverse events among populations of African, Asian, and European descent
Abstract
Objective: Nevirapine is widely prescribed for HIV-1 infection. We characterized relationships between nevirapine-associated cutaneous and hepatic adverse events and genetic variants among HIV-infected adults.
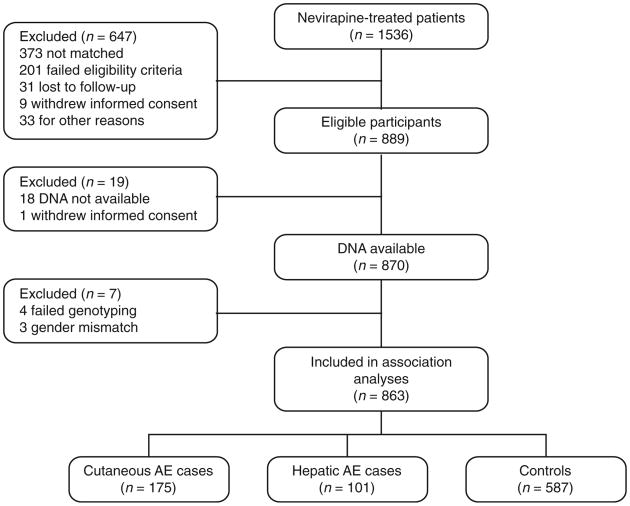
Design: We retrospectively identified cases and controls. Cases experienced symptomatic nevirapine-associated severe (grade III/IV) cutaneous and/or hepatic adverse events within 8 weeks of initiating nevirapine. Controls did not experience adverse events during more than 18 weeks of nevirapine therapy.
Methods: Cases and controls were matched 1: 2 on baseline CD4 T-cell count, sex, and race. Individuals with 150 or less CD4 T cells/μl at baseline were excluded. We characterized 123 human leukocyte antigen (HLA) alleles and 2744 single-nucleotide polymorphisms in major histocompatibility complex (MHC) and drug metabolism and transport genes.
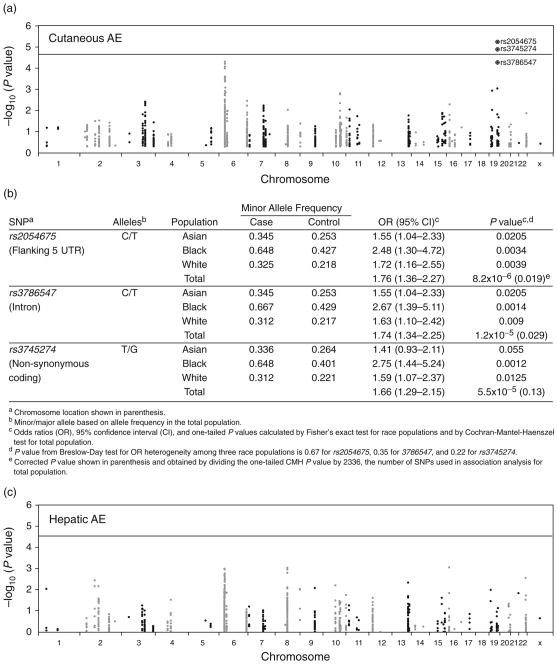
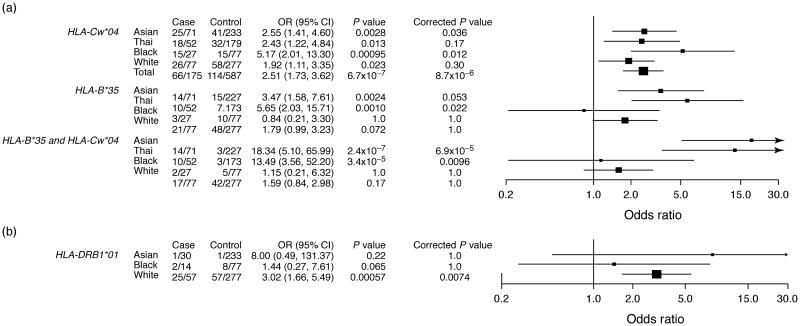
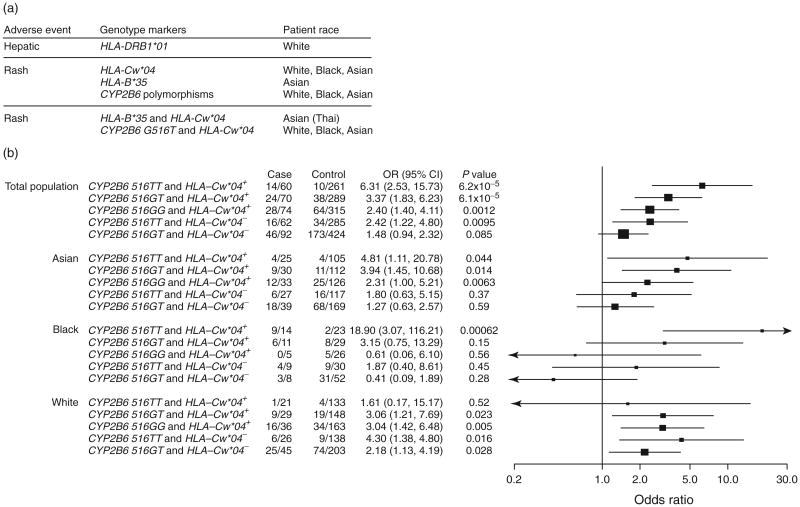
Results: We studied 276 evaluable cases (175 cutaneous adverse events, 101 hepatic adverse events) and 587 controls. Cutaneous adverse events were associated with CYP2B6 516G→T (OR 1.66, all), HLA-Cw*04 (OR 2.51, all), and HLA-B*35 (OR 3.47, Asians; 5.65, Thais). Risk for cutaneous adverse events was particularly high among Blacks with CYP2B6 516TT and HLA-Cw*04 (OR 18.90) and Asians with HLA-B*35 and HLA-Cw*04 (OR 18.34). Hepatic adverse events were associated with HLA-DRB*01 (OR 3.02, Whites), but not CYP2B6 genotypes. Associations differed by population, at least in part reflecting allele frequencies.
Conclusion: Among patients with at least 150 CD4 T cells/μl, polymorphisms in drug metabolism and immune response pathways were associated with greater likelihood of risk for nevirapine-related adverse events. Results suggest fundamentally different mechanisms of adverse events: cutaneous, most likely MHC class I-mediated, influenced by nevirapine CYP2B6 metabolism; hepatic, most likely MHC class II-mediated and unaffected by such metabolism. These risk variants are insensitive for routine clinical screening.
Figures
References
-
- Leith J, Piliero P, Storfer S, Mayers D, Hinzmann R. Appropriate use of nevirapine for long-term therapy. J Infect Dis. 2005;192:545–546. - PubMed
-
- Boehringer-Ingelheim Pharmaceuticals Inc. Viramune( (nevirapine) prescribing information. [Accessed 31 January 2011];2009 http://bidocs.boehringer-ingelheim.com/BIWebAccess/ViewServlet.ser?docBa....
-
- Hoskins JM, Roederer MW, McLeod HL. Nevirapine hypersen-sitivity reaction: will the real HLA please stand up? Curr Opin Mol Ther. 2009;11:226–230. - PubMed
-
- Martin AM, Nolan D, James I, Cameron P, Keller J, Moore C, et al. Predisposition to nevirapine hypersensitivity associated with HLA-DRB1M0101 and abrogated by low CD4 T-cell counts. AIDS. 2005;19:97–99. - PubMed
-
- Gatanaga H, Yazaki H, Tanuma J, Honda M, Genka I, Teruya K, et al. HLA-Cw8 primarily associated with hypersensitivity to nevirapine. AIDS. 2007;21:264–265. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
